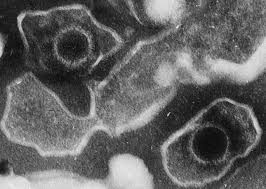
member of the herpesvirus family
ds DNA enveloped virus
nucleocapsid 100 nm in diameter, with 162 capsomers
membrane is derived by budding of immature particles through
cell membrane and is required for infectivity.
genome is a linear ds DNA molecule with 172 kbp
the viral genome does not normally integrate into the
cellular DNA but forms circular episomes which reside in the
nucleus.
the genome is large enough to code for 100 - 200 proteins but
only a few have been identified.
EBV particles
The proteins characterized thus far fall into the following
groups :
A._Latent_proteins
1. EB viral nuclear antigen complex (EBNA) - EBNA is
now known to be a complex of at least 6 proteins ie. EBNA 1-6.
Their functions have yet to be understood but EBNA 1 is thought
to be essential for the maintenance of the episomal state of EBV
in infected cells and binds to the origin of replication. EBNA 1
is expressed in all known virus carrying cells, but its
expression may be lost when a lytic cycle ensues. EBNA 2 has two
phenotypes, A and B, strain A, which is found mainly in
Caucasians, is more efficient in immortalizing B lymphocytes than
strain B, which is mainly found in Africa. However, neither
strains have any specific disease association.
2. Latent membrane protein (LMP) - LMP is thought to be
a membrane associated protein which is found in the virus
particle as well as the infected cells. The structure of LMP
resembles a growth factor receptor which may play a role in the
immortalization process. The transfection of LMP into NIH 3T3
cells causes a tumourigenic phenotype to be expressed.
3. Terminal protein - this new protein family was
described recently but its function is unknown. The terminal
proteins are only expressed when the viral genome is circularized
as its reading frame spans the terminal repeat sequences.
4. Lymphocyte-detected membrane antigen (LYDMA) - LYDMA
is the name given to viral coded proteins in expressed cells
which are recognized by EBV specific Tc cells. LMP and EBNA-2
have been shown to act in such a capacity as antigenic targets
for Tc cells.
B._Lytic_cycle_proteins
1. Membrane antigen (MA) - MA consists of at least 3
glycoproteins, gp 350, gp 250 and gp85, which are present on the
viral envelope and the cell membranes of infected cells. These
molecules mediate the attachment of the virus to the cell and are
antibodies against MA are virus neutralizing.
2. Early antigen complex (EA) - EA is a complex which
is only expressed in infected cells undergoing the lytic cycle.
The functions of the proteins of the EA complex are as yet
unknown.
3. Viral capsid antigen complex (VCA) - the VCA complex
comprises of the structural proteins which make up the viral
capsid and are synthesized late in the lytic cycle.
Man is the natural host for EBV though some primates eg.
tamarins, gibbon, owl monkey and squirrel monkey may be infected
experimentally. In humans the only cell types known to be
infected are (i) squamous epithelial cells, and (ii) B
lymphocytes. These are the only cells which express the receptor
for EBV ie. CR2, the receptor for the C3d component of
complement. The outcome of EBV infection in these cell types are
different. In squamous epithelial cells, a lytic infection occurs
with the production of progeny and cell death. In B cells,
immortalization takes place, with a minority of cells undergoing
the lytic cycle. Until recently, it has not been possible to grow
EBV in squamous epithelial cells.
EBV_Immortalization
Human B lymphocytes are immortalized when infected by EBV in
vitro as well as vivo. The resting B cells undergo blast
transformation with an increase in HLA-DR expression, nuclear
size, and cytoplasmic volume and also the expression of certain
cellular genes eg. CD23. CD23 is also thought to play a role in
the immortalization process. After 36 hours, DNA synthesis is
initiated and cell division takes place. Immunoglobulin is
detected in 1 to 2% of B cells and is secreted into the culture
medium. These early changes seen in B-cells after infection is
similar to those seen after activation by B-cell mitogens.
However, the polyclonal activation of B-cells is totally
independent of T- cells and the immortalization is a permanent
event.
All cells that are immortalized express CD34 (cluster
designation 23) and EBNA. LMP becomes detectable after EBNA at 48
hours postinfection. This viral gene expression (EBNA 1-6, LMP)
is seen in the majority of cells in a lymphoblastoid cell line
and is termed "latent gene expression". A minority of
cells in a lymphoblastoid cell line at any one time enters the
lytic cycle with the resultant production of viral progeny and
cell death. Different cell lines have varying degrees of
permissiveness for viral replication, ranging from <1% in cell
lines derived from umbilical cord cell lines to 15% in the B95-8
cell line derived from tamarin. Most cell lines can be induced by
some agents to produce more virus eg. TPA, anti-IgM Ab. These
agents induce the maturation of the B-cells.
In developed countries, 2 peaks of infection are seen : the
first in very young preschool children aged 1 - 6 and the second
in adolescents and young adults aged 14 - 20. 80 - 90% of the
adult population have been infected by the virus. In developing
countries, infection occurs at a much earlier age so that 90% of
children over the age of 2 are seropositive.
Once infected, a lifelong carrier state develops whereby a low
grade infection is kept in check by the immune defenses. Low
grade virus replication and shedding can be demonstrated in the
epithelial cells of the pharynx of all seropositive individuals.
Furthermore a few EBV-immortalized B-cells can be demonstrated in
the circulation which are continually cleared by immune
surveillance mechanisms. Whether these B-cells are true latent
EBV infected B-cells or cells which become infected as they pass
through Waldeyer's ring in the pharynx is uncertain. EBV is
associated with several diseases state where it may act as the
direct agent or as one of several cofactors. These diseases
include :-
1. Infectious Mononucleosis
2. Burkitt's lymphoma
3. Nasopharyngeal carcinoma
4. Lymphoproliferative disease and lymphoma in the
immunosuppressed.
5. X-linked lymphoproliferative syndrome
6. Chronic infectious mononucleosis
7. Oral leukoplakia in AIDS patients
8. Chronic interstitial pneumonitis in AIDS patients.
Since virus shedding can be demonstrated in the oropharynx of
most seropositive individuals, it is thought that transmission
occurs mainly by the oral route. Thus IM has been dubbed the
"kissing disease". More recently, virus replication has
been detected in vivo in the uterine cervix, thus raising the
possibility of sexual route for the transmission of IM (Similar
to CMV). IM has also been acquired by individuals receiving large
amounts of blood.
Infectious Mononucleosis
Infectious mononucleosis is an acute self-limiting
lymphoproliferative disease resulting from primary infection with
EBV. Primary EBV infection is usually subclinical in childhood
but where the infection is delayed until adolescents and young
adulthood (15 - 25), there is a 50% chance that the person
infected will develop IM. EB virus enters the body through the
mouth and establishes a productive infection in the pharyngeal
epithelial cells. B-cells become infected and are disseminated
throughout the body via the bloodstream. During acute primary
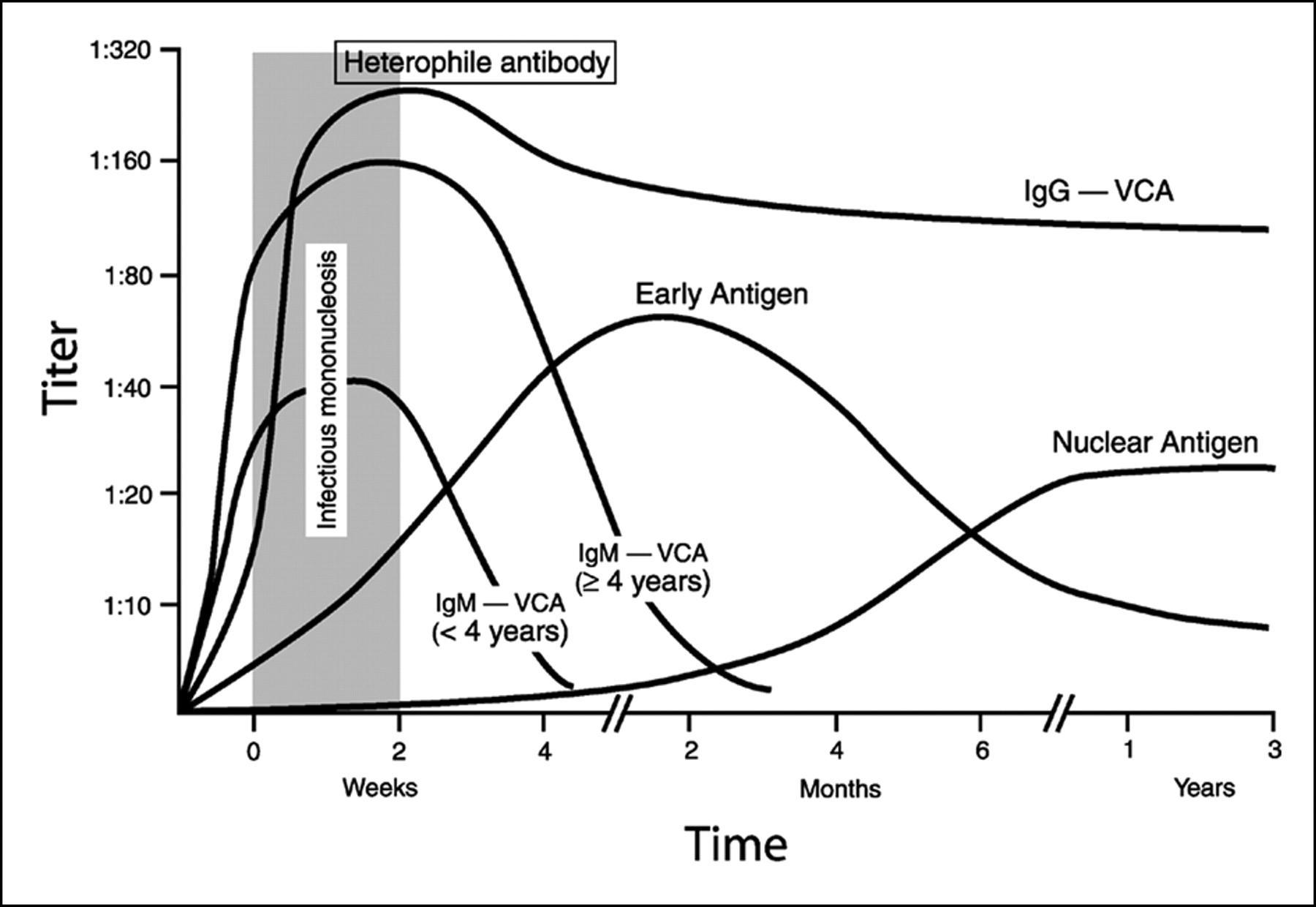
infection, IgA, IgM and IgG to VCA as well as IgG to EA(D) and MA
are induced. Antibodies to EBNA, a latent phase protein, are not
usually detectable in the serum until the convalescent period.
Heterophile antibodies appear early in IM, but their relationship
to the virus is unclear. A variety of autoantibodies are also
found in IM, which includes cold agglutinins, rheumatoid factor,
anti-nuclear antibodies and antibodies to smooth muscle. These
antibodies are thought to be due to the polyclonal activation of
B-cells. They are usually transient and harmless. The atypical
lymphocytes characteristically seen in IM are CD8 cytotoxic
lymphocytes that react against EBV-infected B cells in a non-MHC
restricted manner. These Tc cells probably play an important role
in recovery from the virus infection.
Clinical Features - The incubation period is not known
as the source of infection is rarely recognized.
Characteristically IM begins with a sore throat and swelling of
the neck, accompanied by fever, malaise, sweating, chills,
headaches, stiff neck, anorexia and vague abdominal discomfort.
The sore throat occurs in 80 - 90% of patients and is usually
mild in nature and clears in 7 - 14 days. Occasionally, gross
tonsillar enlargement may lead to pharyngeal obstruction.
Secondary infection of the pharynx with B-haemolytic
streptococcus occurs in 25% of cases. Less commonly, patients may
present with jaundice, cough, myalgia or symptoms of one of the
neurological complications of IM. Lymphadenopathy is present in
the majority of cases, the cervical lymph nodes are most commonly
involved but generalized lymphadenopathy may occur which may last
for several weeks.
Splenic enlargement and tenderness occurs in 50 - 60% of
patients, and hepatomegaly occurs in 15 - 25% of patients.
Clinically apparent jaundice appears in 5 - 10% of cases. Fevers
of 38 - 40oc are commonly present during the first 2
weeks of IM. Pharyngitis and palatal petechiae occur during the
first week of illness which may be accompanied by a gray-white
membrane. Periorbital oedema may also be present. 2 forms of
rashes occur in IM, a morbilliform eruption which lasts 24 - 48
hrs and a maculopapular rash which occurs following treatment
with ampicillin in virtually 100% of patients treated. Signs of
rare complications such as meningitis and encephalitis may be
present. IM is rare in children and when it occurs, the disease
is usually mild. In the elderly, the onset is often insidious and
occasionally bizarre. The disease can be serious with hepatic,
renal and CNS involvement. IM during pregnancy is not associated
with any deleterious effects on the fetus. However, rare cases of
fatal lymphoproliferative disease in pregnant women who develop
IM has been reported. IM usually lasts for several weeks.
Recovered patients occasionally complain of recurrent attacks of
fatigue typical of the "persistent viral fatigue
syndrome". Some patients suffer relapses of IM like
illnesses within one year following the initial attack, with a
positive heterophil antibody test. The exact nature of these
relapses are unclear at present.
Immunocompromised patients - Where primary EBV
infection occurs in immunocompromised patients, particularly
after organ transplantation, it may result in abnormal disease
with GI symptoms and/or signs of renal graft rejection and
failure. Some of these primary infections go on to develop into
lymphoproliferative disease and lymphoma.
Complications - IM is usually a benign and
self-limiting disease. Certain morbid complications may arise
which account for 30 deaths per annum in the US. These
complications include :-
1. CNS - CNS complications include meningitis,
encephalitis and the Guillain-Barre syndrome. These
complications may precede, accompany or postdate IM by
several weeks. Recovery is usual. Although CNS disorders may
occur as the sole manifestation of an EBV infection, most
cases arise during the course of IM.
2. Hepatic - almost all IM patients have deranged
LFTs, overt jaundice is uncommon (5-10%), and complete
recovery is the rule. More severe cases include massive
hepatic cirrhosis and Reye's syndrome.
3. Splenic rupture - this is a very rare
complication of IM and when it occurs, urgent surgery is
required.
4. Pharyngeal and tracheal obstruction - these may
occur due to massive enlargement and oedema of the tonsils
and adenoids. A short course of steroids is indicated
5. Immunological complications - these include
haemolytic and aplastic anaemia, thrombocytopenia,
hypogammaglobulinaemia, agranulocytosis and
haemophagocytosis. EBV induced autoantibodies may be involved
in these cases.
6. Chronic IM - rarely, chronic cases of IM occurs
where symptoms persists for years and death may result from
lymphamatous disease. In these cases, there is the
persistence of the acute profile of IM, with elevated titres
of IgG against VCA and EA-D antigens. There is an absence of
antibodies against EBNA 1 and a positive monospot test. High
titres of virus can be isolated from throat washings.
Diagnosis - the laboratory diagnosis of IM is usually
made by the heterophil antibody test, which had been reported to
be 98% sensitive for IM. However, false negatives occur commonly
in patients under the age of 5 years and anti-VCA IgM testing
should be carried out in those instances.
Treatment - the management of IM is mainly supportive.
The sore throat may be extremely painful and regular analgesics
are needed. Some physicians regularly treat cases of IM with
corticosteroids but others prefer to reserve them for severe
cases. Acyclovir has been given to patients with IM but did not affect the
course of the disease significantly in those with uncomplicated disease.
Burkitt's lymphoma (BL) occurs endemically in parts of Africa
(where it is the commonest childhood tumour) and Papua New Guinea
and is restricted to areas with holoendemic malaria. BL also
occurs sporadically throughout the world. However, whereas almost
100% of African BL is associated with EBV, only 12% of cases of
sporadic BL are associated with EBV. The evidence that EBV is
involved in the pathogenesis of BL is as follows ;-
1. Multiple copies of EBV genome can be demonstrated in
the monoclonal tumour cells of BL. EBV MA and EBNA-1 antigens
can be detected from all tumour cells and furthermore,
infectious EBV particles can be recovered from tumour cell
lines.
2. All patients with BL have antibodies to EBV antigens.
Furthermore, BL patients are shown to have much higher levels
of such antibodies than comparable seropositive subjects.
Elevated levels of anti-VCA may be used for screening
purposes for BL as there is a 30 fold increase in risk of
developing BL in those children with an anti-VCA titre of two
doubling dilutions or higher than the general population.
3. EBV is able to transform human B-lymphocytes in vitro.
4. EBV can cause tumours in subhuman primates.
Lymphoid cell lines can be grown from BL biopsy materials but
they differ from the cell lines derived from in vitro
transformation in that BL cell lines are monoclonal in nature
whereas in vitro derived cell lines are polyclonal. Also BL
derived cell lines have a greater malignant potential. BL cells
show a reciprocal translocation between the long arm of
chromosome 8 and chromosomes 14, 2 or 22. These translocations
result in the c-myc oncogene being transferred to the
Immunoglobulin heavy chain gene region (14), the light kappa (2)
or lambda regions (14). These regions are thought to be
transcriptionally active and results in the deregulation of the
c-myc gene. It is uncertain whether EBV actually causes these
translocations or that these translocations have already occurred
by the time of infection and thus further malignant
transformation by EBV. The latter is more likely.
Cofactors - although EBV is ubiquitous, EBV associated
BL occurs almost exclusively in parts of the world where malaria
is holoendemic. In areas where malaria had been successfully
eradicated, the incidence of BL has declined dramatically. Also
BL is rare in children with the sickle cell trait which is known
to protect against malaria. The actual mechanism through which
malaria act as a cofactor is uncertain. There is evidence that
chronic infection by malaria leads to a decrease in cellular
immunity and thus immunosurveillance. Another possibility is that
malaria leads to a sizable increase in the pool of B cells that
can be infected.
Clinical Features - BL usually occurs in children aged
3 - 13 years with a peak incidence at 6 - 7 yrs. In areas where
BL is endemic ie. some parts of Africa and New Guinea, the
incidence is around 15 per 100000 children aged 5 - 10 years and
is the commonest childhood malignancy. BL is more common in boys
than girls and arises extranodally typically in the area of the
jaw. The tumour is usually found to be multifocal at
presentation, the other sites involved being the bone marrow, GI
tract, ovaries and breast. BL is usually a highly malignant
tumour with death supervening within 4 months of onset in
untreated cases, although self-cures have occasionally been
reported. The tumour is, however highly sensitive to
chemotherapy.
Diagnosis - In endemic areas, BL can often be diagnosed
from the typical clinical features. Histology of biopsy specimens
should reveal a poorly differentiated lymphocytic lymphoma. The
tumour can be stained with antibodies to lambda light chains
which should reveal a monoclonal tumour of B-cell origin. In over
90% of cases, the cells express IgM at the cell surface.
Treatment - BL is very sensitive to chemotherapy, one
dose of cyclophosphamide often being sufficient to cause complete
remission of the tumour mass. The prognosis is good after a full
course of treatment if given early.
Prevention - Prevention can theoretically be achieved
by the eradication of malaria, or by vaccination against EBV.
Where the eradication of malaria have been achieved eg. in parts
of New Guinea, the incidence of BL had dropped dramatically.
NPC is a malignant tumour of the squamous epithelium of the
nasopharynx. It is very prevalent in S. China, where it is the
commonest tumour in men and the second commonest in women. The
tumour is rare in most parts of the world, though pockets occur
in N. and C. Africa, Malaysia, Alaska, and Iceland. The most
undifferentiated form of the tumour is always associated with EBV
whereas the rarer, more differentiated forms are not consistently
so. The evidence that EBV is involved in the pathogenesis of NPC
is as follows :-
1. Multiple copies of the EBV genome can be detected in
the malignant cells of 100% of undifferentiated NPC. All the
malignant cells express EBNA-1 and some have been reported to
express LMP. Furthermore, infectious EBV particles can be
recovered from NPC cell lines.
2. 100% of sera from undifferentiated NPC patients have
high-titre antibodies to EB-viral antigens. As in BL,
antibodies against VCA are at a 10 times geometric mean
titre. IgG and IgA levels against EA (D) and VCA rise as the
disease progress and may be used for screening and monitoring
purposes. VCA and EA (D) IgA are also uniquely found in the
saliva of NPC patients.
Cofactors - NPC is a genetically restricted tumour,
being most common in the Southern Chinese, with intermediate
frequency in some Negro and Mongoloid races and rare in
Caucasians. Studies have shown that first-generation immigrants
from S. China retain the high incidence of the disease, with the
later generations showing a decline in incidence. This suggests
that environmental as well as genetic factors are involved. NPC
is especially associated with certain HLA haplotypes eg.HLA A2.
More genetic linkage studies demonstrated the presence of NPC
susceptibility genes near the MHC genes. Environmental factors
are thought to play a role, in particularly the consumption of
salted fish and foods containing nitrosamines.
Clinical Features - NPC occurs at a rate of 98 per
100,000 of the population of Southern China and is more common in
men than women. The EBV associated undifferentiated type arises
mainly in younger patients whereas the more differentiated types
occur in older patients and constitute the bulk of the sporadic
cases. The tumour most commonly arise in the posterior wall of
the nasopharynx in the fossa of Rosenmuller, where it often
remains silent and metastasizes to the local lymph nodes. The
most common presentation of NPC is bilateral enlargement of the
glands in the neck. The primary tumour may be very small and
difficult to locate. Less frequently, the patient may present
with the symptoms of invasion by the primary tumour eg. nasal
obstruction, postnasal discharge, epistaxis, partial deafness and
cranial nerve palsies. If untreated, the disease is rapidly fatal
due to the development of laryngeal and pharyngeal obstruction.
Diagnosis - the diagnosis of NPC is usually made on
histological examination of biopsy material. 3 types of NPC are
recognized on histological appearance :-
1. a well differentiated SCC
2. a non-keratinizing carcinoma
3. an undifferentiated carcinoma
Serum antibodies to EBV antigens can be used to confirm the
diagnosis and monitor the progress of the disease. Recent studies
have demonstrated the value of testing for persistent high levels
of serum IgA to VCA in screening for early lesions of the
disease. It is hoped that early lesions can be diagnosed in this
way and treated, and then monitored.
Treatment - NPC is difficult to treat surgically
because of the early metastasis to regional lymph nodes. The
tumour is resistant to chemotherapy and radiotherapy is the
treatment of choice. However, because the tumour usually presents
late, the prognosis is poor with a 5 year survival rate of 20%.
It should in theory be possible to prevent the development of NPC
with the use of an EBV vaccine at an early age.
EBV_Infection in the Immunocompromised
After primary infection, EBV maintains a steady low grade
latent infection in the body. This latent infection is normally
kept in check by the cellular defenses which, if impaired later
in life, may lead to the reactivation of the virus to cause
clinical disease. In a few cases, lymphoproliferative lesions and
lymphoma may develop. These lesions tend to be extranodal and in
unusual sites such as the GI tract or the CNS.
1. X-linked Lymphoproliferative Syndrome
Many families are known where the male members are unable to
mount an effective cell-mediated immune response to EBV
infection. The defective gene is located on the X chromosome.
This condition accounts for half of the fatal cases of IM, the
other half being sporadic with an equal age distribution.
Clinically the affected male members are healthy until primary
EBV infection occurs. The course of the disease can be either (i)
fulminating and rapidly fatal, or (ii) progress on to a chronic
phase which may culminate in a fatal B-cell lymphoproliferative
disease, variously described as immunoblastic lymphoma,
plasmacytoma and American Burkitt's lymphoma. These tumours often
occur in the CNS or GI tract.
Many abnormal laboratory findings have been reported in X-LPS,
including defects in NK cell activity and a defect in EBV
specific T cell cytotoxicity. The pattern of antibodies to EBV
antigens is also abnormal, with high titres of anti-VCA and EA
antibodies and low EBNA antibodies. This pattern is identical to
that seen in many immunosuppressed states and probably reflects
increased viral replication leading to raised VCA and EA with
decreased killing of infected cells resulting in low anti-EBNA
titres. Female carriers show a milder derangement of antibody
pattern but with normal EBV specific T-cell killing.
2. Transplant Recipients
Post Transplant Lymphoproliferative Disorder (PTLD) is thought
to be a lymphoproliferation of EBV infected B-cells arising in
the setting of over immunosuppression. The patients at risk are
those who encounter EBV as a primary infection during the
post-transplant course. The proliferation may be seen anywhere
lymphoid tissue presides, although in lung transplant recipients,
presentation in the allograft is relatively common.
Histopathological manifestation appears as nodular sheets of
atypical lymphoid cell which are not dissimilar to Non-Hodgkins
lymphomas. Some cases are similar to lymphomatoid granulomatosis
or T-cell rich B-cell lymphomas with a large subset of reactive
T-cells. Reduction in immunosuppression often results in
regression of PTLD.
It is well known that there is an increased incidence of
malignancy following organ transplantation and maintenance
immunosuppression. Malignant lymphoma accounts for 20% of such
malignancies. Lymphomas have been reported to develop in 1 - 13%
of patients following renal transplantation, 7.3% of cardiac
transplants. Post transplant lymphomas have also been reported in
bone marrow and heart/lung transplant recipients. The tumours
tend to occur in the CNS, the GI tract, or in the transplanted
organ. Most can be shown to carry the EBV genome and the cells
express EBNA. High titres of antibodies to EA and VCA are
present, which suggests increased virus replication. In around
50% of those developing EBV-associated lymphoma, there is
evidence of recent primary infection.
It has been shown that the immunosuppressive therapy following
transplantation reduces the CMI to EBV. Indeed, cessation of
immunosuppressive had been accompanied by the regression of the
lymphomas in some cases. Lymphomas in the immunocompromized are
usually of the B cell type and classified as non-Hodgkin’s
large cell lymphoma. They are usually extranodal, in the brain,
gut and the transplanted organ and arise in 1-10% of transplant
recipients. Around 80% of these tumours carry EBV genome and
express EBNA. The large cell lymphomas express the same antigens
as the lymphoblastoid cell lines, including the 2 viral oncogenes
and cd 23. The majority of these tumours are monoclonal in
nature.
EBV-associated tumours occur frequently in patients with AIDS.
Lymphomas are the second commonest malignancy in AIDS patients.
However, not all lymphomas in AIDS patients are associated with
EBV. The EBV associated tumours are (i) primary lymphoma of the
brain and, (ii) Burkitt's lymphoma (50% of these tumours are
similar to the African type and associated with EBV, whilst the
other 50% are EBV genome negative). Recently, oral hairy
leukoplakia has been described in HIV- seropositive individuals,
forming multiple characteristic lesions on the lateral side of
the tongue. DNA hybridization studies have shown active EBV
replication in these lesions. In infants with AIDS, a lymphocytic
infiltration of the lungs termed chronic interstitial pneumonitis
in which the lymphocytes carry the EBV genome. However, it is
thought that the syndrome is probably due to the direct action of
HIV rather than EBV.
Laboratory_Diagnosis of EBV Infections
1. Infectious Mononucleosis - the classical finding in
IM is the presence of atypical mononuclear cells in the blood.
Lymphocytes would account for more than 50% of leucocytes present
and of these, 20% are atypical. Atypical lymphocytes may also be
seen in infections by CMV, hepatitis, influenza B, and rubella,
but they are most prominent in IM. Abnormal LFTs are also present
in the majority of patients. The diagnosis of IM may be suspected
on clinical grounds and the findings of atypical lymphocytes,
However, a firm diagnosis can only be made on serological
testing. 2 types of serological tests are generally used for the
diagnosis of IM.
The Heterophil antibody test is commonly called the
Paul-Bunnel test, or the Monospot test (if done on slides). This
test detects an antibody which causes agglutination of red blood
cells from another species. False negative heterophil Ab test
results occur and are more common in children under 14 years,
especially under the age of 5 years. A possibility is that
priming exposure to the unknown "heterophil antigen"
has not taken place in very young children and thus no secondary
response will arise on polyclonal stimulation. False positive
heterophil Ab results are fewer in number than false negative
results. Positive heterophil Ab results may last more than 6
months after the onset of IM and can occur in asymptomatic
primary infection. This may be responsible for some of the
"false" positive results.
IgM to VCA by indirect immunofluorescence is the best
serological test available for the diagnosis of IM. However, this
test is time consuming and results may vary between different
laboratories. Also false positive results in the IgM may result
from the cross linking between EBV specific IgG and anti-IgM
conjugate by rheumatoid factor. If rheumatoid factor is present
in the serum, it should be absorbed with staphylococcal protein A
before testing. For these reasons, most laboratories rely mainly
on the heterophil antibody test. A pre- illness specimen is
rarely available to demonstrate a rise in IgG antibodies to VCA.
High levels of VCA IgG are not diagnostic of acute infection. VCA
IgM is generally used in the diagnosis of acute infection and IgG
as an immune status screen.
Testing for EBNA antibodies may be of use in the window
period. Anti-EBNA-1 antibodies do not usually arise until
convalescence. Anti-EBNA-2 antibodies arise earlier in the
illness and fall to low or undetectable levels during
convalescence. The absence of EBNA- antibodies should not be
regarded as diagnostic for IM as they are often undetectable in
chronic IM, and conversely, they may be present soon after the
onset of IM. Another possible confirmatory test is EBV-IgG
avidity. The elution principle (avidity-index) is generally used
for VCA-IgG.
Time course of various anti-EBV antibodies
2. Chronic IM - signs and symptoms of chronic IM range
from fever, Pharyngitis, malaise, myalgia, and lymphadenopathy to
potentially life-threatening problems such as anemia,
thrombocytopenia, hupoglobulinaemia, and pneumonitis. Onset of
chronic IM follows acute IM and may be due to impaired
cell-mediated response to the virus. To meet the criteria for a
diagnosis of chronic IM, three conditions need to be satisfied;
(1) the symptoms should have persisted for at least 12 months (2)
onset of persistent symptoms should have been preceded by a
proven case of IM; (3) there should be evidence of active EBV
infection . Highly elevated VCA and EA antibodies are often
observed (>1024), EBNA-2 antibodies are frequently higher than
those of EBNA-1 (the reverse of the situation is found in normal
seropositive individuals), a positive heterophil antibody result
may be seen, and more rarely, anti-VCA IgM may be detected.
Similar antibody profiles have been observed in patients
suffering from post-viral fatigue syndrome. It may be that some
PVFS patients were, in fact suffering from chronic IM.
3. Burkitt’s Lymphoma - histology of biopsy
specimens should reveal a poorly differentiated lymphocytic
lymphoma. The tumour can be stained with antibodies to lambda
light chains which should reveal a monoclonal tumour of B-cell
origin. In over 90% of cases, the cells express IgM at the cell
surface. The presence of EBV in tumour cells can be demonstrated
by hybridization or the detection of EBNA-1. However, both these
methods are technically demanding and therefore a diagnosis of BL
is usually made on clinical and histological grounds. Children
with BL have highly elevated titre of antibodies to EBV which may
decrease following treatment and remission. Therefore, the
determination of antibody levels may have a role in the
monitoring of treatment. Although EBV serology might be of value
in the early diagnosis of BL, such monitoring is not feasible on
financial and practical terms.
4. Nasopharyngeal Carcinoma - the diagnosis of NPC is
usually made on histological examination of biopsy material.
However, the presence of EBV DNA and EBNA-1 can be readily
demonstrated. Serum antibodies to EBV antigens can be used to
confirm the diagnosis and monitor the progress of the disease,
especially serum IgA to EA, VCA and ENA-1.. Recent studies have
demonstrated the value of testing for persistent high levels of
serum IgA to VCA in screening for early lesions of the disease
and also for monitoring treatment.
5. X-linked Lymphoproliferative syndrome - the
diagnosis of XLPS is much the same as for IM. In addition,
EBNA-positive infiltrating lymphocytes can often be detected in
post mortem or biopsy material. Serological studies of XLPS
families commonly reveal a carrier state in healthy female
relatives as evidenced by elevated EA and/or VCA titres. In such
cases, genetic counseling may be given.
6. Post transplant lymphomproliferative disease - it is
possible to detect EBV-DNA and EBNA in most of these lesions. The
demonstration of EBNA positive cells is probably the most
suitable method. Unlike BL and NPC, other latent antigens, ie.
all the EBNAs and LMPA are expressed. The majority of
EBV-associated post transplant lymphoproliferative lesions appear
to occur following primary EBV infection. Serological diagnosis
of primary infection is usually made retrospectively on sera
taken for other purposes, as these patients rarely exhibit
symptoms of IM. It may be possible to demonstrate a
seroconversion. Patients who were seropositive prior to the
transplant may have an antibody profile suggestive of
reactivation.
Vaccine Development
A vaccine against EBV which prevents primary EBV
infection should be able to control both BL and NPC. Such a
vaccine must be given early in life. Such a vaccine would also be
useful in seronegative organ transplant recipients and those
developing severe IM, such as the male offspring of X-linked
proliferative syndrome carriers. The antigen chosen for vaccine
development is the MA antigen gp 340/220 as antibodies against
this antigen are virus neutralizing. Inoculation of cotton top
tamarins by purified gp 340/220 was able to protect the animals
by subsequent virus challenge. However to date, there is no licensed vaccine
available against EBV.