A Picornavirus, now classified as a heptovirus, formerly
known as enterovirus 72
Naked icosahedral ssRNA virus
Genome consists of a single +ve stranded RNA with 7478
nucleotides, which codes for 4 proteins ;- VP1 VP2 VP3 VP4
1 serotype only, although there are 4 genotypes
virus can be propagated in primary marmoset cell culture and
also in vivo in chimpanzees and marmosets
Electronmicrograph of hepatitis A virus particles.
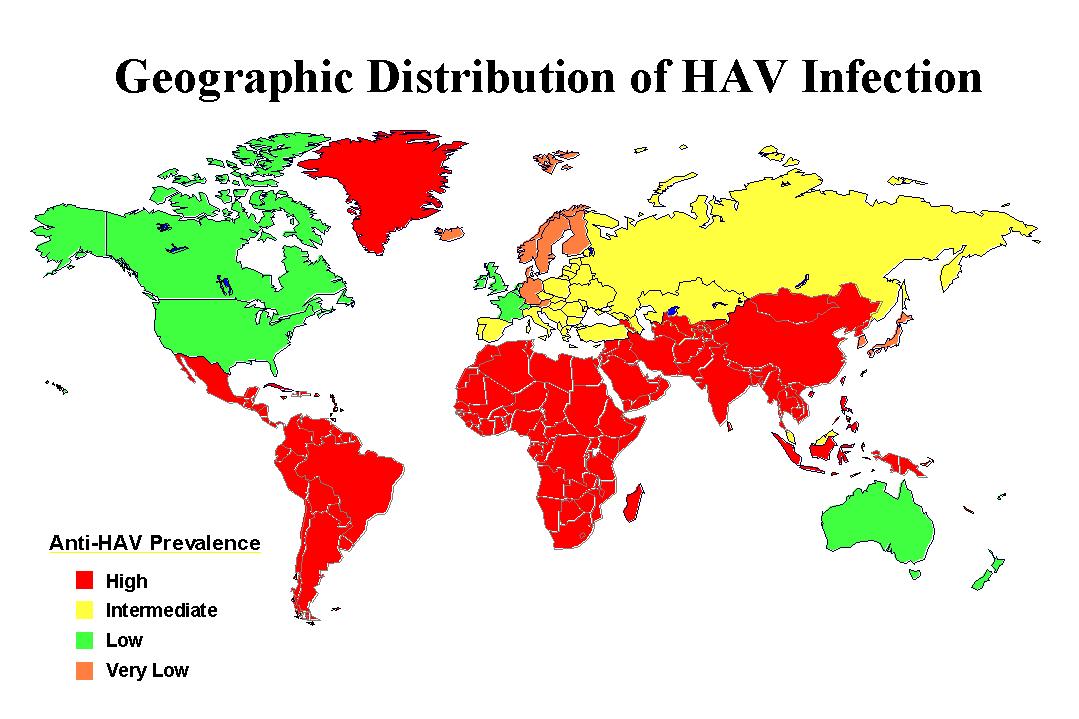
EPIDEMIOLOGY
Hepatitis A occurs endemically in all parts of the world, the
exact incidence is hard to estimate because of the high
proportion of subclinical infections. At least 1.5 million new
cases are reported each year. While the actual incidence in
developed countries is decreasing, the infection is almost
universal in developing countries. Hepatitis A virus (HAV) is a
faecal-oral pathogen and transmission is particularly associated
with faecally contaminated food and water. Shellfish is
particularly notorious as a vehicle for the spread of HAV. In a
recent epidemic in Shanghai following a clam festival, there were
over 500,000 cases. Infection is particularly common in
conditions of poor sanitation and overcrowding, institutions for
the mentally handicapped are particularly vulnerable. Many
foodborne outbreaks can be traced to poor hygiene in infected
food handlers who were shedding large amounts of virus during the
incubation period. The source of the outbreak can often be traced
to uncooked food or food that has been handled after cooking.
Until recently, about 50% of young adults in the UK had evidence
of past infection, but as in the case of other industrialized
countries, the incidence is rapidly decreasing so that hepatitis
A is rapidly becoming a disease of young adults rather than
children in these countries. HAV is frequently acquired from
travelers from areas where HAV infection is of a low prevalence
to an area where it is hyperendemic.
The incubation period is 3 - 5 weeks (15 - 40 days), with a
mean of 28 days. Spread is faecal-oral although bloodborne
infection is possible in theory (this was achieved experimentally
in volunteers). All age groups are susceptible to HAV. In areas
where HAV is hyperendemic, hepatitis A is an childhood infection
where the infection is usually subclinical or mild. In developed
countries where the overall incidence is decreasing rapidly, the
infection is now more commonly seen in adults where the disease
is usually more serious.
PATHOGENESIS
The pathological changes are common to all types of viral
hepatitis, with parenchymal cell necrosis and histiocytic
periportal inflammation. Rarely in cases of fulminant hepatitis
there is massive necrosis. Liver enzymes such as AST and ALT are
elevated as a result of release by damaged liver cells. Elevation
of these enzymes may often be the only abnormality found in
individuals with asymptomatic and anicteric infections who are
tested because of known exposure. Serum bilirubin may be
elevated, especially in most cases of symptomatic infections and
bilirubin may be found in the urine. The leucocyte count is
usually normal but sometimes atypical lymphocytes are seen.
Clinical_Features
Following an incubation period of around 4 weeks, at the end
of which virus particles are excreted in the faeces, there is an
acute onset of non-specific symptoms such as fever, chills,
headache, fatigue, malaise, and aches and pains. A few days
later, anorexia, N+V and right upper abdominal pain appear,
followed by the onset of jaundice with pale stools and dark
urine. With the appearance of the jaundice, there is usually a
subjective improvement of symptoms. The jaundice deepens for the
first few days and then persists for 1 - 2 weeks. Convalescence
may be prolonged and complete recovery in adults usually takes
place within a few months. In children the infection is commonly
asymptomatic or the prodromal phase mild or absent. The mortality
rate is very low for hepatitis A and no carrier state exists.
Complications of hepatitis A include prolonged cholestatic
jaundice which responds to corticosteroid therapy, and relapsing
disease which occurs in 6 to 10% of patients and lasts 16 to 40
weeks. Relapsing disease appears to be immunologically mediated
and must not be treated by corticosteriods. Extrahepatic
complications include a rash and arthropathy.
LABORATORY_DIAGNOSIS
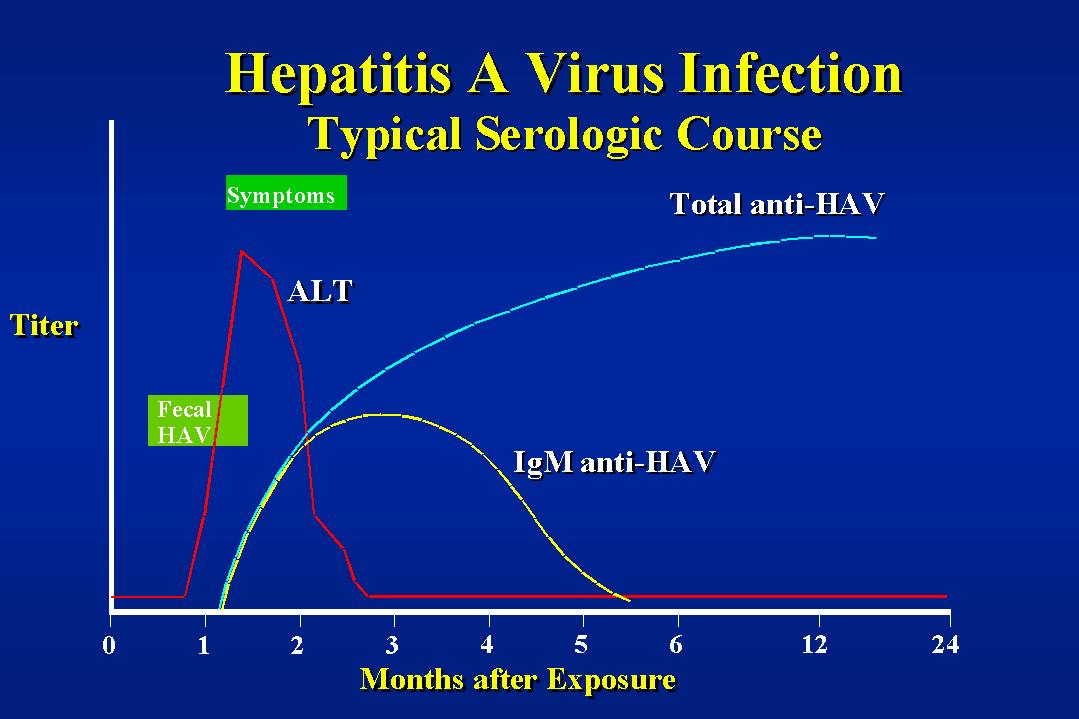
1. Detection of the virus or antigen ;- The virus can
be detected in the faeces up to 2 weeks before the appearance of
the jaundice and up to 2 weeks afterwards. However by the time
that jaundice appears, viral titres in the faeces are already at
a low titre and so in practice EM if the stools is rarely of
diagnostic value. Hepatitis A virus can also be detected in the
serum, saliva, urine and semen although transmission is unlikely
to take place via these routes. There had been anecdotal reports
of hepatitis A transmitted through blood transfusions. RT-PCR is the assay of
choice for detecting Hepatitis A virus.
2. Serology ;- This is the method of choice for the
diagnosis of acute hepatitis A. A variety of ELISAs and RIAs are
available. The detection of specific IgM is diagnostic of recent
infection. (IgM may be found 45 - 60 days after the onset of
symptoms). Serum IgG is used in determining the immune status of
the individual before the prescription of immunoglobulin for
foreign travel.
PREVENTION_AND_CONTROL_OF_HEPATITIS_A
The control of infection is difficult as the height of faecal
excretion occurs during the late incubation period and the
prodromal phase. Isolation of cases is not strictly necessary as
a control measure. The spread of HAV can be reduced by simple
hygienic measures and the sanitary disposal of excreta. HNIG
containing at least 100 i.u./ml of anti-HAV given before exposure
to the virus or early during the incubation period will prevent
or attenuate a clinical illness. Immunoglobulin does not always
prevent infection and the excretion of HAV. HNIG is used most
commonly for close personal contacts of patients with hepatitis A
and has also been successfully used in controlling outbreaks in
institutions. However since maximal virus excretion has already
passed by the time clinical symptoms appear, HNIG is probably of
little value in preventing infection in a household although it
may in theory attenuate the course of the disease in contacts.
The RVL policy is to discourage the prescribing of HNIG in the
case of family contacts. However consideration should be given to
protect people at risk in an institution. There HNIG would only
be given to adults where the consequence of infection is much
more severe than children. The doses used are as follows ;-
Under 10 years 250 mg
10 years and over 500 mg
HNIG is used for prophylaxis for travelers to areas with a
high endemicity. In practice, hepatitis A occurs 100 times more
frequently in travelers than typhoid fever. The protection is
valid for 6 months, after which the administration should be
repeated ;-
Period
Abroad Age Dose
0 - 2 months
< 10 125 mg
>= 10 250 mg
3 - 5 months
< 10 250 mg
>= 10 500 mg
Hepatitis A Vaccine
"HAVRIX" (SmithKline Beecham) is a
formaldehyde-inactivated vaccine prepared from HAV HM 175 grown
in human diploid cells. It is available in prefilled syringes
containing a turbid, white suspension. Each 1 ml dose contains no
less than 720 ELISA units of hepatitis A viral protein absorbed
on aluminium hydroxide adjuvant. The vaccine is recommended for
those at increased risk of infection. This includes those
traveling to, or living in, medium or high endemicity areas. Other
high risk groups include recent close contacts of infected
individuals and potential contacts of cases such as childcare or
healthcare workers. In the event of case contact, HNIG should be
given simultaneously with HAVRIX in different sites.
"HAVRIX" is given im and the regimen consists of 2
doses of 1ml of vaccine spaced 2 weeks to 1 month apart and
provides anti- HAV antibodies for at least 1 year. In order to
obtain more persistent immunity of up to 10 years, a 1 ml booster
dose is recommended between 6 to 12 months following the initial
dose.
"HAVRIX" should not be given to those
with severe febrile infections. In haemodialysis patients and in
immunocompromized subjects, adequate antibody titres may not be
obtained after the primary immunization course and such patients
may therefore require administration of additional doses of
vaccine. "HAVRIX" can be given with recombinant
Hepatitis B vaccine and interference is unlikely to occur with
other inactivated or live vaccines. Although the risks in
pregnancy are probably negligible, the vaccine is not recommended
in pregnancy unless there is a definite risk of hepatitis A.
Adverse reactions are usually mild and confined to the first few
days after vaccination. The most common complaints are soreness,
erythema and induration at the injection site.