The Australia antigen was discovered by Blumberg et al. in
1965 which was recognized to be associated with hepatitis B.
Previously hepatitis B was diagnosed on the basis of infection
occurring 60 - 180 days after the injection of human blood or
plasma fractions or the use of inadequately sterilized needles.
Hepatitis B is the only human representative of a family of DNA
viruses (Herpadnaviradae) of which related viruses have been
found in woodchucks, Peking ducks and ground squirrels.
Properties
Double stranded DNA virus,the + strand not complete
Replication involves a reverse transcriptase.
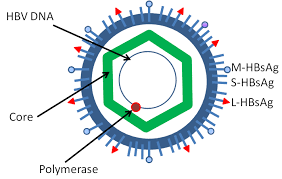
Complete Dane particle 42 nm
28 nm electron dense core, containing HBcAg and HBeAg
The coat and the 22 nm free particles contain HBsAg
At least 4 phenotypes of HBsAg are recognized;
adw, adr, ayw and ayr.
The HBcAg is of a single serotype
It has not yet been possible to propogate the virus
in cell culture.
Structure of Hepatitis B Virus particle
Electron microscopy of hepatitis B virus-positive serum
reveals 3 morphologically distinct forms of particles ;-
Small 22nm spherical or tubular forms comprise of
virus surface proteins which are synthesized in excess of the
42 nm complete virions.
Complete 42 nm virion (Dane particle). The HBsAg
differs from the HBsAg found in the 22 nm particles in that
pre-S1 epitopes are present.
The 27 nm nucleocapsid comprises of the DNA genome
surrounded by a second protein, the HBcAg. A third antigen,
the HBeAg is found in the soluble forms in virus-positive
sera and is related to the core antigen.
The genome comprises of circular DNA and the positive strand
is incomplete (50 - 80%). The genomes of a variety of isolates of
hepatitis B ave been sequenced. Although there is some variation
in sequence (up to 12%), the genetic organization is conserved.
There are 4 open reading frames derived from the same strand (the
incomplete + strand). The first reading frame codes for the
proteins making up HBsAg, the second for HBcAg, the third for the
viral polymerase, the function of the fourth is unknown.
The major protein of HBsAg is 226 a.m.u. long and is found in
both glycosylated and non-glycosylated form (gp 27 and p24). The
gene region it is translated from is called S. However larger
proteins can be translated from 2 initiation codons that are
situated further upstream in the pre-S region. The pre-S2
proteins (gp33 and gp36) appear to be minor components of both 42
nm virion and 22 nm subunit particles. The largest pre-S1
proteins (p39 and gp42) appear to be found only in the complete
42 nm virions. A domain on the pre-S1 region may be responsible
for the attachment of the virion to the hepatocyte. The major
HBsAg protein also carries a pair of mutually exclusive
subdeterminants, d or y and w or r. 4 principle phenotypes of
HBsAg are recognized ; adw, adr, ayw and more rarely ayr. These
phenotypes show differing geographical distribution e.g.. ayw
predominates in N. Europe, N. America and Australia ; adr in China
and Japan.
The core protein is the major component of the nucleocapsid.
HBeAg may be generated from the core protein by proteolytic
cleavage. The P reading frame codes for the viral polymerase. The
function of the product of the X reading frame is uncertain but
appears to act as a transcriptional activator which may enhance
the expression of other proteins. . Variants of HBV have been
described in Taiwan, France, Italy and Senegal which shares a few
epitopes with the envelope of classical HBV but no cross
reactivity with the core or e antigen. There is no anti-HBc
response and no cross protection from the anti-HBs Ab.
Replication ;- The replicative process of the
hepadnaviruses is unique among animal DNA viruses in that reverse
transcription is involved. After absorption, the virus is uncoated
and the single-stranded region of the genome is repaired by the
viral polymerase. Viral RNAs are transcribed some of which act as
mRNAs, others act as templates for the synthesis the progeny
genomes where the process of reverse transcription is involved.
Epidemiology
Blood and blood products are the main routes through which the
virus is transmitted. Only a very small amount of blood is needed
for transmission (down to 0.00004 ml intradermally). Any
technique that allows the transfer of blood or serum from one
individual to another is potentially likely to transmit HBV. HBV
infection is especially common amongst IV drug abusers. Before
the advent of screening, many cases occurred following blood
transfusion. It is also particularly common amongst homosexuals
where the practice of anal intercourse is particularly traumatic
and frequently results in bleeding. Cases have been reported
following acupuncture, tattooing and ear piercing.
HBV is a known occupational hazard. The risk to health workers
following accidental inoculation is 6 - 20%. Health personnel in
renal dialysis units are particularly vulnerable. It is striking
that infected professionals often develop severe disease whereas
their immunocompromised do not, suggesting that an
immunopathological mechanism may be involved in the pathogenesis
of the disease. Many infected health workers on the haemodialysis
units do not recall any accidental inoculation.
It has become clear that HBV is not spread exclusively by
blood and blood products. Under certain circumstances, the virus
is infective by mouth. It is endemic in closed institutions such
as homes for the mentally handicapped and prisons. The virus is
also found in semen, vaginal discharges, breast milk and serous
exudates such as the CSF and these have been implicated as
possible vehicles of transmission. The presence of HBV antigens
has been reported in urine, faeces, bile, sweat and tears but has
not been confirmed. There have been cases of family outbreaks of
hepatitis B where no known exchange of blood has occurred. The
entrance of the virus through the membranes of the eye or mouth
must be a possible route of transmission. All biological fluids
from a HBV infected individual must be treated as potentially
infectious. Although HBsAg has been detected in mosquitoes and
bed bugs, there is no convincing evidence for replication of the
virus in these insects. The role of arthropod vectors in
uncertain although mechanical transmission of infection must be a
possibility.
Clustering of HBV infection also occurs within family groups,
but does not appear to be related to genetic factors and does not
reflect maternal or venereal transmission. HBV does not normally
infect the fetus but the baby is at risk of infection during the
birth process. The perinatal transmission of HBV is an important
factor in maintaining the high level of carriers and thus the
prevalence of HBV infection in some regions, notably China and
S.E Asia. The risk of transmission to the fetus may reach 50 -
60%, though it varies from country to country and appears to be
related to ethnic groups. The risk is greatest if the mother has
a history of transmission of infection to previous children or
has a high titre of HBsAg or e antigen. There is also a
substantial risk of perinatal infection if the mother had acute
hepatitis B in the second or third trimester of pregnancy or
within 2 months of delivery. Although HBV can infect the fetus in
utero, this appears to be rare and is generally associated
with antepartum haemorrhage and tears in the placenta. The
mechanism of perinatal transmission is uncertain. It probably
occurs during or shortly after birth as a result of a leak of
maternal blood into the baby's circulation or of its ingestion or
inadvertent inoculation. Most children infected during the
perinatal period become persistent carriers. 70 - 90% of infants
born to e +ve mothers become carriers.
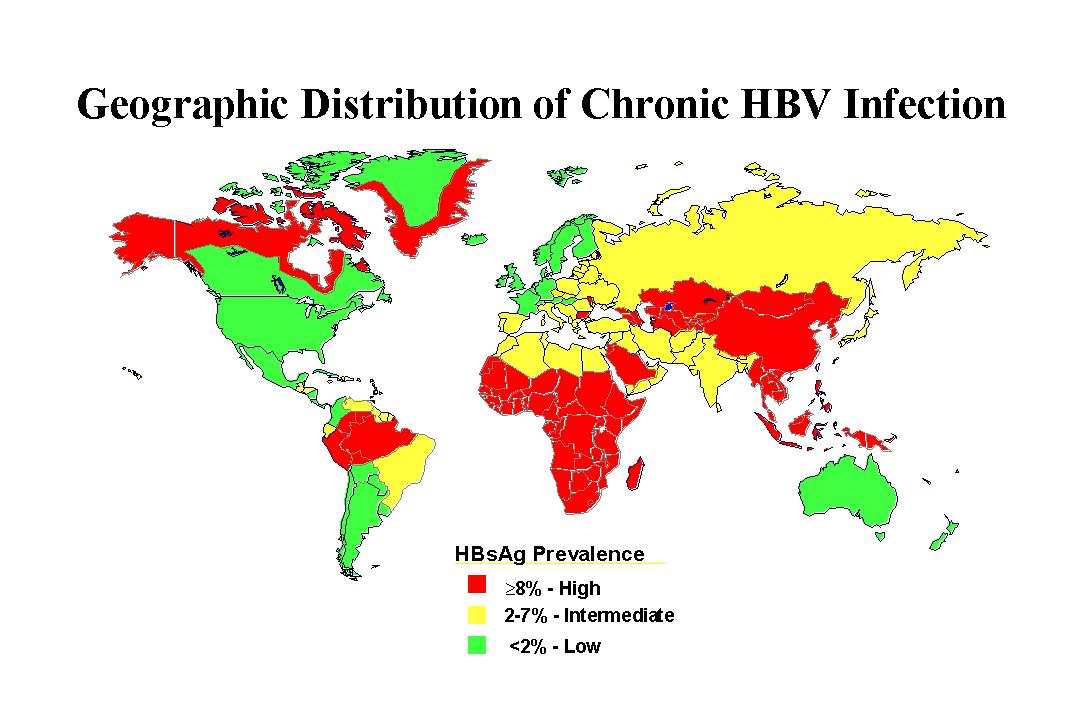
Hepatitis B infection is found worldwide but the prevalence
varies enormously between different countries. It is estimated
that one-half of the world population has experienced infection
and there are 350 million chronically infected individuals.
Hepatitis B is responsible for 1.5 million deaths per year.
Around 40% of chronically infected individuals will die as a
result of their infection. The high carrier rate and the high
rate of perinatal infection appears to be the mechanism for
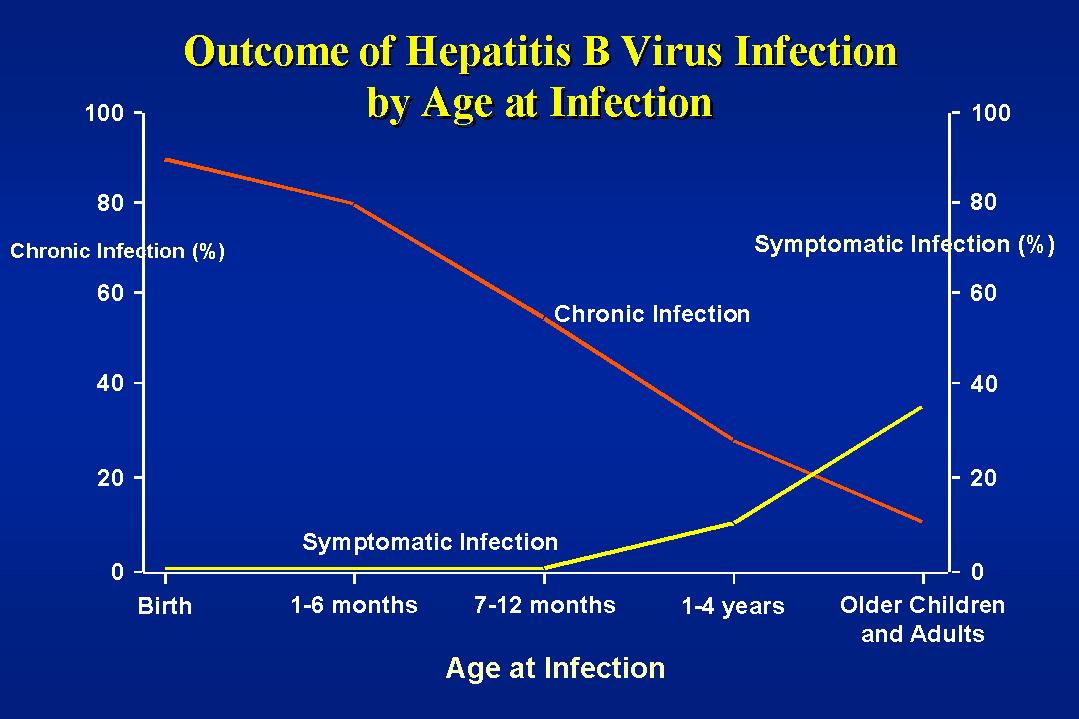
maintaining the high prevalence rate in some countries. In high
prevalence areas, infection in infancy is very common,
particularly acquired from the carrier mothers at birth. The
earlier in life the infection, the more likely is persistent
carriage to be the outcome. The result is that the carrier rate
in the adult population is 10 - 20% and almost all the remainder
of the population is immune. In areas of intermediate prevalence,
infection is also common in childhood but is usually horizontal
between children. This may be due to the fact African HBV carrier
mothers are less likely to be e +ve than their Oriental
counterparts and thus less likely to transfer HBV perinatally.
The carrier rate in adults is 2 - 10% and a quarter to half the
population is immune. In low prevalence areas, infection in
childhood is rare, the carrier rate is low, 0.1 - 0.5% with a low
prevalence of natural immunity in the general population being in
order of 2 - 6%. The UK having one of the lowest rates.
E.Europe
N and W.Europe
Mediterranean Parts of China
N.America USSR
SW.Asia
S.E.Asia
Australia
S.America
Tropical Africa
HBsAg
0.2 - 0.5% 2 -
7% 8
- 20%
Anti-HBs
4 -
6%
20 - 55% 70 - 95%
Neonatal
infection
Rare
Frequent Very
Frequent
Childhood
infection
Infrequent
Frequent Very
Frequent
The Carrier State
The carrier state is defined as persistence of the HBsAg in
the circulation for more than 6 months. The carrier state may be
lifelong and may be associated with mild liver damage varying
from minor changes in liver function to chronic active hepatitis
and cirrhosis and hepatocellular carcinoma. The carrier state is
more likely to occur if the infection occurred earlier in
childhood rather than adults. It is more frequent in males and
more likely to occur in those with acquired or natural immune
deficiencies. Approximately half the carriers are e antigen
positive. A carrier state is established in 5 - 10% of infected
adults. The e antigen is also more likely to be positive in
younger carriers.
Pathogenesis
Infected hepatocytes are characteristically enlarged and their
cytoplasm has a ground glass appearance. HBsAg is found
associated with the endoplasmic reticulum, core particles
containing HBcAg are present in the cell nuclei. Due to large
antigenic load present in hepatocytes and in the serum, together
with the knowledge is more likely to be asymptomatic or mild in
the immunocompromised, it has been postulated that liver injury
may result from immune mechanism. Necrosis of hepatocytes results
in scattered focal inflammatory response with macrophage and
lymphocyte infiltrations together with portal inflammation and
endophlebitis of the central veins. In more severe cases, lines
of necrosis extends from the portal tracts to the central veins
and this often precedes chronic hepatitis and cirrhosis.
Those who become asymptomatic carriers may either have normal
liver histology or may show chronic liver inflammation that is
recognized as chronic persistent hepatitis. This normally
resolves within months or years of acute infection. Some may
develop chronic periportal hepatitis which correlates clinically
with chronic active hepatitis and continuing patchy necrosis with
fibrosis is likely to lead to the major disruption in liver
architecture characteristic of cirrhosis. It takes around 4 to 5
years for cirrhosis to develop. Some carriers may go on to
develop hepatocellular carcinoma.
Clinical Features
The incubation period for hepatitis B is 6 weeks to 6 months
ie. 40 - 180 days (ave. 90 days or 3 months). As with hepatitis A
the clinical picture is very variable, although the disease is on
the whole more severe than hepatitis A. Asymptomatic and minor
non-specific infections are common. The onset is insidious, with
a non-specific prodrome consisting of fever, fatigue, nausea,
diarrhoea, anorexia, chills, discomfort or pain in the right
hypochondrium. The prodrome may be present for 1 - 3 weeks before
the jaundice becomes apparent. Arthritis and urticaria are common
and may sometimes precede the jaundice and these are thought to
be due to circulating immune complexes. The onset of the jaundice
is insidious and is accompanied by the darkening of urine and
pale stools. In children, the onset of symptoms is more abrupt
and the icteric phase shorter. GI disturbances predominate with
vomiting, abdominal pain and ketoacidosis being usual. Although
urticaria and arthritis are uncommon in children, other immune
complex phenomena, particularly glomerulonephritis and papular
acrodermatitis are relatively common. Recovery normally takes 6
to 12 weeks after the onset of illness. About 0.1% of patients
presenting with acute hepatitis B develop fulminant hepatitis
with death from liver failure. The mortality of acute HBV
infection increases with age and also with the presence of other
disorders.
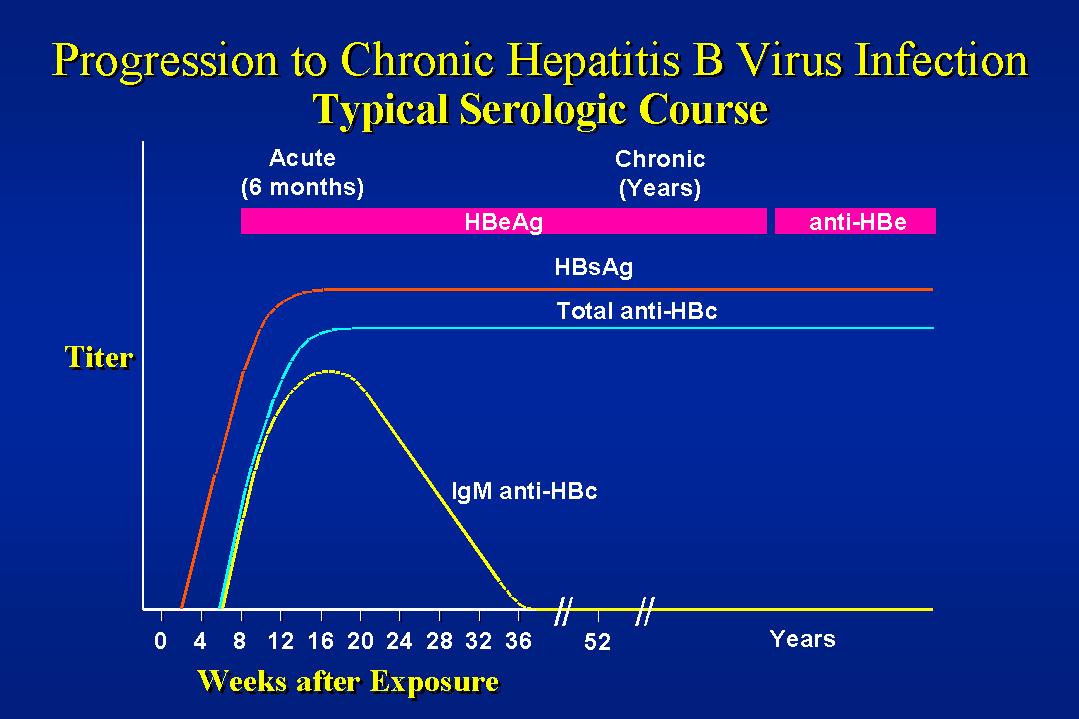
The Immune Response and the Carrier State
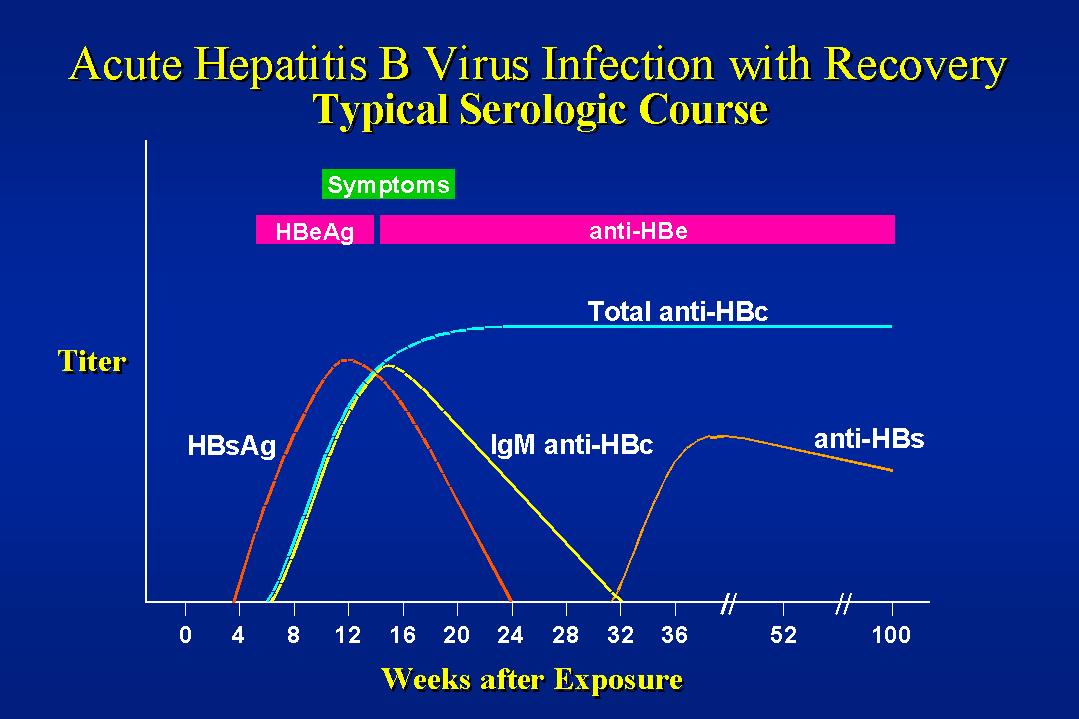
Following HBV infection,the first marker to appear is HBsAg,
which is evident 2 to 8 weeks before the appearance of the
jaundice and biochemical evidence of liver damage. Next to appear
are the markers of the virion, such as virus-specific DNA
polymerase activity, the viral DNA and the soluble antigen,
HBeAg. Although HBcAg is present, it is not detectable in the
serum due to the early appearance of anti-HBc. Anti-HBc is found
2 - 4 weeks after the appearance of the surface antigen, at
around the same time as the development of the signs and
symptoms. In acute infections, clearance of the virus is marked
by the disappearance of HBeAg and the appearance of anti-HBe.
Later during convalescence, HBsAg also disappears with the
appearance of anti-HBs. CMI to HBsAg appears near the end of the
acute phase of hepatitis and appears to be mainly responsible for
the disappearance of HBsAg. In contrast, anti-HBs does not appear
until months after the termination of the clinical illness. It is
noteworthy that in chronic HBsAg carriers specific CMI is
generally decreased and circulating anti-HBs is not demonstrable.
However, on electron microscopic examination of the patients'
sera reveal HBsAg - anti-HBs immune complexes. An increase in
anti-HBs is clearly correlated with immunity. In the case of
approx. 10% of infected adults and a much larger percentage of
perinatally infected children, the immune system fails to clear
the infection and a carrier state develops (The carrier state is
defined as the persistence of HBsAg in excess for more than 6
months). The carrier state may be divided into 2 phases ;-
(1) Virus replication continues and the patient is
positive for HBeAg and the markers of the virion (viral DNA
and DNA polymerase). Although HBeAg correlates with the
presence of the virus and thus infectivity, in some cases,
virus replication declines to very low levels and
seroconversion to anti-HBe may occur. Therefore detection of
viral DNA and DNA polymerase (by PCR or hybridization or the
endogenous polymerase reaction) is a more reliable indicator
of viral replication and infectivity. (It is not uncommon for
HBV DNA to be detected in e -ve carriers nor is it uncommon
for HBV DNA to be undetectable in e +ve carriers.) During
this phase of chronicity, replicative forms of HBV DNA may be
detected in the liver. Levels of virus replication may
decline until this is eliminated with the development of
anti-HBe. Rarely there will also be seroconversion to
anti-HBs.
(2) In this second phase, HBsAg persists in the absence of
active virus replication. HBV DNA is now integrated
chromosomally in the hepatocytes. and HBsAg is produced
following the transcription of this integrated DNA. This
integration of the HBV DNA into the host cell chromosome may
be a stage in the development of hepatocellular carcinoma.
The integration of the HBV DNA is thought to occur at the
time of seroconversion of e Ag.
In general e +ve carriers have a high infectivity whereas e
-ve carriers have a much reduced or absent infectivity. Over a
number of years, it is quite common to see e +ve carriers
seroconvert with the development of anti-e Abs and then progress
onwards to lose their HBsAg and develop anti-HBs. The rate for
the reversion of the carriers to being naturally immune is around
2% per year. In chidren born to carrier mothers, girls are much
more likely to seroconvert than boys although both sexes are just
as likely to be infected and become carriers initially. It is not
unusual for people who were naturally immune with anti-HBs to
lose their anti-HBs and develop HBsAg in their blood (especially
Haemophiliac patients with AIDS). It is not certain whether this
is due to reinfection or the reactivation of the virus.
Chronic HBV carriage may take the form of chronic active
hepatitis (CAH) or chronic persistent hepatitis (CPH) or minimal
hepatitis. The distinction can only be made on histological
examination of the liver. CAH is far more common in e +ve
carriers as it is indicative of active viral replication.
Cirrhosis and hepatocellular carcinoma (HCC) is thought to be
more common in e -ve carriers. It was suggested that those e -ve
carriers who had a prolonged e +ve stage are more prone to
developing cirrhosis and HCC. It was reported that nuclear DNA is
commonly detected alone in the late phase of HBV infection, which
represents either integrated fragments or supercoiled HBV DNA,
whereas cytoplasmic and nuclear HBV DNA is commonly detected in
the early phase of the illness and CAH, which is indicative of
active viral replication.
HBV is essentially hepatotropic but HBV DNA has been detected
in other sites such as the peripheral leucocytes, the bone marrow
and spleen. The viral DNA is usually in episomal form and is
rarely integrated. These findings have implications for virus
transmission and also for the possible recurrence of hepatitis B
infection in patients who have cleared infection in the liver, in
particular patients with AIDS who had had anti-HBs following an
acute infection in the past but become HBsAg positive again.
Individuals infected with both hepatitis B and hepatitis C are
prone to prolonged disease, cirrhosis and hepatocellular
carcinoma.
LABORATORY_DIAGNOSIS
A battery of ELISAs and RIAs are now available for the
diagnosis of specific serological markers of HBV infection.
+ +
- +
+ - Acute
hepatitis B or persistent carrier state
+ +
- -
+ - Persistent
carrier state
+ -
+ +/-
+ - Persistent
carrier state
- -
+ +/-
+ + Convalescence
- -
- -
+ + Recovery
- -
- +
- - Infection
with HBV without detectable HBsAg
- -
- -
+ - Recovery with
loss of detectable anti-HBs
- -
- -
- + Immunization
without infection. Repeated exposure to antigen without infection,
or recovery from infection with loss of detectable anti-HBc
During the incubation period, HBsAg is the first serological
marker to appear. This occurs 2 to 8 weeks before biochemical
evidence of liver dysfunction or the onset of jaundice. The
antigen persists throughout the course of the illness and is
usually cleared from the circulation during convalescence. Next
to appear is the viral DNA polymerase and the e antigen. The e
antigen is a distinct soluble antigen that is located within the
core and correlates closely with the no, of virus particles and
the relative infectivity. Anti-HBc is found in the serum 2 - 4
weeks after the appearance of the surface antigen and is always
detectable during the acute early phase of the illness. Core IgM
become undetectable several months after the onset of
uncomplicated acute infection, but core IgG persists for many
years, possibly for life. The next antibody to appear is the
anti-e. In general, the presence of anti-e is associated with low
infectivity of the serum. Anti-Hbs is the last marker to appear
late during convalescence.
In general, detection of HBsAg is used for the diagnosis of
acute infection and the screening for carrier status. HBeAg is
used to assess the potential infectivity of carriers and
antibodies to specific antigens indicate past infection and are
of value in monitoring progress. Core IgM is of value in
diagnosing recent infection in those who have lost detectable
antigen and in whom antibodies have not become apparent (termed
the diagnostic window). It is possible to get cases where
anti-HBs has disappeared whilst anti-HBc persists. It is also
possible to have a situation where anti-HBs is present with no
anti-HBc with no history of immunization. This may occur in a
situation when the person is continually exposed to minute
amounts of HBV which is insufficient to set up an infection. In
this manner, the patient becomes immune to HBV.
The presence in the serum gene products of the pre-S1 and
pre-S2 regions has been found to be associated with high levels
of replication. Pre-S proteins have also been found in the liver.
The presence of pre-S1 proteins in the serum and in the liver
correlates closely with HBV DNA and on cessation of viral
replication, pre-S1 is no longer detectable. Antibodies to pre-S2
have been reported as markers of viral clearance and recovery.
Furthermore anti-pre-S2 neutralize the infectivity of HBV. These
antibodies may be important in the clearance of circulating HBV
virions and the termination of infection ; their absence in
patients with chronic active hepatitis may explain why infection
persists. Other tests which may be of value include ;-
(1) The detection of HBsAg-IgM immune complexes -
This has been shown to be of value in predicting the outcome
of an acute HBV infection in the sense of whether the patient
is likely or not to go onto becoming a carrier. HBsAg-IgM
immune complexes should only be present for a few weeks after
which they become undetectable. If HBsAg-IgM immune complexes
persists for more than a few weeks, then the patient is
likely to become a carrier.
(2) Serotyping of the HBsAg - This can be done by
the use of monoclonal antibodies. Such typing may provide
useful information on the epidemiology of a particular
outbreak. However, its usefulness is limited by the low no.
of strains of HBsAg so that typing of HBsAg will never
provide as much information as phage typing for S.aureus.
HBV-DNA Testing - the determination of HBV DNA has
increasing become a routine part of HBV testing, especially for carriers on
antiviral therapy and also those with symptoms who are HBeAg -ve i.e. suspected
of being infected by core escape mutants. A variety of commercial tests are
available that are based on different molecular techniques, including DNA-hybrdization,
branched DNA, PCR, Real Time qPCR and LCR. For the purpose of monitoring the response to
therapy, it is essential that the same assay is used throughout the whole
period.
Management
There is no specific therapy for acute hepatitis B. To date, there is no
conclusive evidence that early treatment with antiviral agents speeds recovery
or reduce the chance of developing chronicity, although trails are ongoing. General measures which apply to
all forms of acute hepatitis are as follows ;-
Bed rest, hospital admission if required
Diet - A good general diet is desirable.
Drugs - Although corticosteroids have been advocated
in viral hepatitis. Current evidence is that they do not aid
recovery and they may have serious side effects.
Cases of fulminant hepatic failure - there is no
specific treatment but certain measures should be instituted
as soon as possible once cerebral changes occur including (i)
Nitrogen exclusion diet (ii) Neomycin (iii) Mannitol to
reduce cerebral oedema (iv) Close supportive measures.
The patient should be monitored by serological tests at regular
intervals to check whether on not he has developed carrier status. If
so, then treatment with antiviral agents may be considered (see below)
Antiviral Treatment of Chronic Infections
In chronic hepatitis B, treatment may be given to
suppress viral replication and the progression of disease. Therapy is not
usually recommended for patients with normal enzymes. Therapy is recommended for
patients with evidence of active damage to the liver such as raised liver
enzymes and evidence of damage seen on liver biopsy. The American Association for
the Study of Liver Diseases (AASLD) also recommends the treatment of patients
with compensated and decompensated cirrhosis and measurable HBV DNA regardless
of e Ag status. Six agents had been recommended by the FDA for treatment of
chronic HBV infection: 2 types of interferons and 4 types of
nucleoside/nucleotide analogues.
Interferon Therapy
It has been postulated that chronic carriage of HBV is due
mainly to inadequate production of interferon and the failure of the body to
respond to interferon in the presence of acute HBV infection. Two
preparations of interferons are currently available: Alpha-Interfron (Intron
A) and Peginterferon (Pegasys). In In early clinical trials, interferon therapy
is associated with HBeAg loss in 30-40% of patients, and in approximately 10%
lost HbsAg altogether. If a patient loses HBeAg loss during interferon therapy,
HBsAg loss follows therapy in approximately 80% of patients followed for a
decade. In addition, improved survival, complication-free survival, and a
reduction in the frequency of hepatocellular carcinoma have been reported in
those who responded to interferon. Interferon therapy is more effective in
patients with low-level HBV DNA 100,000–40 million copies per mL, elevated ALT (esp
if >200 IU/mL), immunocompetence, normal liver function (albumin, bilirubin and
coagulation), and acquisition of infection in adulthood. Early studies suggested
that the efficacy of interferon was low in patients with pre-core-mutant HBV
infection (HBeAg negative strains), but recent observations have renewed
interest in interferon for this indication. Emerging data on PEG interferon may
result in the first line use of PEG products alone or in combination with oral
agents. However, interferon requires inconvenient injection therapy, is
associated with a lot of side effects, and is no better than lamivudine in terms
eAg seroconversion. Morover, it isof limited value in certain subgroups although
it is the only medication that offers a chance at a complete cure.
Interferon-alpha (Intron A) is given by injection
several times a week for six months to a year, or sometimes longer. The drug
can cause side effects such as flu-like symptoms, depression, and headaches.
Approved in 1991 and available for both children and adults.
Pegylated Interferon (Pegasys)-
peginterferon is is modified form of interferon that has been approved for
the treatment of HBV and HCV. It has a similar but larger chemical
structure than interferon-alpha. This improves the efficiency of the drug so
that it only needs to be injected once weekly, usually for six months to a
year. The drug can cause side effects such as flu-like symptoms, depression
and other mental health problems. Approved May 2005 for adults.
Other Antiviral Agents
Lamivudine (Epivir-HBV) - This was the first antiviral
agent licensed for the treatment of chronic hepatitis B and therefore have the
most data available. It is taken orally once a day for at least a year, and is
approved for use in both adults and children. Lamvivudine has now been licensed for the treatment of chronic
hepatitis B. Clinical trials with lammivudine as monotherapy have
demonstrated that lamvivudine causes a significant reduction in
HBV DNA, enhances HbeAg seroconversion, and reduces progression
of fibrosis. There are almost no side effects. However, YMDD drug
resistant mutants begin to emerge after 36 weeks of therapy. So
that at the end of the first year, 15% of strains are resistant,
and at the end of the second year, 35% are resistant. However, it
appears that the mutant virus is less replicative-competent. Because of the
problem with the emergence of mutants, there is intense interest and study on
the use of combination therapy.
Adefovir dipivoxil (Hepsera)--- Approved only for
adults, it is taken once a day as an oral tablet. Studies have shown that use of
adefovir does not induce as much resistance as lamivudine. Clinical trials are
being planned in children. In summary, Lamivudine and adefovir have both been
shown to be safe and convenient to take, achieve a 30+% HBeAg loss,
histologic improvement in the majority of patients (not limited to HBeAg
responders, as is the case for interferon), Importantly, lamivudine
requires longer-duration therapy and is associated with the emergence of viral
variants that are rarely seen with adefovir therapy.
Entecavir (Baraclude)--- Approved by the FDA March 30,
2005 fro adults in whom the virus is active and replicating. It is taken as an
oral tablet or solution once daily. Entecavir is one of the most potent agents
to date with very little side effects reported. Entecavir can also be used
in patients with a resistant virus who have failed lamivudine therapy. HBV is
much less likely to develop resistance to entecavir.
Telbivudine (Tyzeka, Sebivo) is a pill taken once a
day, with almost no side effects for up to one year. Studies have shown that it
rapidly and profoundly suppresses HBV levels. Approved in October 2006 by the
FDA for adults. Several clinical trials have reported it to be more effective
than lamivudine and adefovir.
Liver transplantation may be an option if the liver is severely damaged.
Prevention
Active_Immunization
Active immunization against HBV is indicated for groups at
increased risk of acquiring this infection. These groups include
medical personnel involved in the care of patients who are
potential carriers, laboratory staff, people working in high risk
institutions such as those for the mentally handicapped.
Individuals requiring repeated blood transfusions and/or blood
products and those who may require haemodialysis in future. The
spouses, other sexual contacts, and other family members in close
contact of patients with acute hepatitis B or those who are
carriers. Women in areas of the world where the carrier rate is
high may be considered for immunization in view of the risk of
transmitting the infection to their offspring. Infants born to
mother with acute infection or carriage should be immunized.
Young infants, children and susceptible persons living in areas
of the world with a high prevalence of carriers should also be
considered.
There were 2 types of vaccine licensed, each containing 20
mg/ml of HBsAg. One is purified from the plasma of carriers, the
other is a recombinant protein produced by yeast cells. As of
1991 only the vaccine produced from yeast is licensed. The
vaccine has a good overall response rate of 90% (More recent
studies suggest that this figure is over-optimistic. The actual
percentage of vacinees who do not or make a poor response is
probably in the region of 15 -20%). However it is less effective
in the immunocompromised and the elderly. 10 to 15% of those aged
over 40 do not respond and only 60% of those undergoing
maintenance haemodialysis respond. Non-responders should be
considered for a booster dose but even then, the response is
likely to be poor and HBIG may be necessary should exposure to
Hepatitis B occurs. People who are immunodeficient or on
immunosuppressive therapy may be given larger doses and/or
additional doses of vaccine. The duration of antibody is thought
to be 3 to 5 years. Advice on the need for further booster dose
have yet to be formulated, but individuals at high risk may wish
to determine their Ab levels periodically. If it falls below
100Iu/L then a booster dose should be given. Suitable intervals
for testing Ab levels are 1 year and 5 years after vaccination.
Recommendations
The vaccine takes up to 6 months to confer adequate protection
and recipients should be advised so. The vaccine should not be
given to people who are HBsAg positive, naturally immune or
suffering from acute hepatitis B. The vaccine may be given to HIV
positive individuals. Screening for HBV markers may be undertaken
in a population where the antibody prevalence is high. Groups of
individuals considered for vaccination include ;-
(1) Health Care Personnel
This include all hospital personnel who may come into
contact with hepatitis B patients and those working in the
units for the mentally handicapped
Laboratory workers and mortuary technicians.
Health workers on secondment to areas of the world
where there is a high prevalence of HBV
(2) Susceptible Patients
Patients undergoing haemodialysis - as the response to
vaccination is poorer in immunocompromised or older patients,
it is recommended that patients with chronic renal damage
should be immunised as soon as possible before their disease
develops to the stage when they require dialysis or
transplant. b
Patients on entry to institutions dealing with the
mentally handicapped.
Haemophiliacs and those receiving regular blood
transfusions or blood products.
(3) Close Contacts ;-
The spouses or other sexual partners of carriers of hepatitis
B (Intimate contacts of individuals suffering from acute
hepatitis B and sexual contacts of highly infectious carriers
should be given HBIG followed by or simultaneously with active
HBV immunisation.)
Consideration should also be given to the following groups of
people who are at higher risk of contracting HBV than the general
population ;-
Police and Emergency Services
People visiting other countries for lengthy periods
Highly promiscuous individuals, especially homosexuals
Inmates of prisons
IV drug abusers
(Morticians and Embalmers
Dosage and Regimen
The basic regimen consists of 3 doses of vaccine. The first
dose is given at an elected date, the second 1 month after the
first and the third dose 6 months after the first. An accelerated
schedule has also been used with the recombinant vaccine (eg. for
travelers) with the third dose given 3 months after the first
followed by a booster in 1 year.The vaccine is given i.m. but may
be intradermally or s.c. for haemophiliac patients. Post
vaccination antibody screening should be done 2 - 4 months after
the course of injection.The vaccines are well tolerated generally
but rarely symptoms such as fever, rash, malaise, myalgia and
arthralgia had been reported. The vaccine can be given to
pregnant women at risk as HBV infection carries a severe risk for
the mother and the newborn. Vaccination should be postponed in
individuals suffering from febrile illnesses. Approximately 50%
of individuals will seroconvert (produce anti-HBs of greater than
10 miu/ml) after the first dose, and up to 90% after the second
dose. The third dose does not increase numbers of seroconversions
significantly and it is meant to be a booster.
Passive Immunization
Hepatitis B immunoglobulin (HBIG) is prepared from the pooled
plasma with high titre of anti-HBsAg. It may confer temporary
immunity of 1 to 3 months if administered under certain
conditions. It is used to protect an individual after a single
acute exposure to HBV. It is most effective if given within 48
hours of exposure and it should not be given after 7 days
following exposure. The dose used is around 600 i.u. in adults
and it should be administered as soon as possible after exposure
and it is generally recommended that 2 doses of HBIG should be
given 30 days apart. HBIG is also given to infants born to e +ve
carrier mothers together with active immunization at the same
time. It should be given within 12 hours of birth. The chance of
the baby developing carrier status is reduced by about 70%. More
recent studies using combined active and passive immunization
indicate an efficacy approaching 90%.
Hepatitis B immunoglobulin (HBIG) is normally used in
combination with hepatitis B vaccine to confer passive and active
immunity after exposure. The vaccine and HBIG are given
simultaneously at different sites. It has been shown that HBIG
does not suppress the active immune response to the vaccine. A
single dose of 500 Iu for adults and 200 Iu for the newborn is
sufficient for healthy individuals. If infection has already
occurred at the time of administration, HBIG can reduce the
severity of the disease and prevent the development of the
carrier state in many individuals, especially in infants born to
mother carriers. Groups requiring post- exposure protection are
;-
Infants born to mother who are persistent carriers,
especially those who are eAg positive. The nature and size of
the risk at birth varies from persistent carriage in 80 - 90% of
infants of HBeAg positive mothers to the less frequent occurrence
of hepatitis B infection in infants of anti-HBe positive mothers
(around 10%). In countries with high prevalence, HBIG is sometimes given to all
babies born to mothers who are HBsAg positive irrespective of HBeAg status.
In countries with low prevalence such as the UK, the infants at risk should be identified. The
following antenatal mothers should be screened ;- (i) All ethnic groups
other than Caucasian, though Caucasians from Southern and Eastern Europe
should also be considered, and (ii) All those with a personal or family history of occupation
suggestive of an increased risk of exposure to HBV.
Infants born to mothers who are HBsAg positive as a result
of recent infection, particularly if HBeAg is detectable and
anti-HBe is not.
Combined active and passive immunisation is recommended for
infants at risk. The first dose of the vaccine should be given at
birth or as soon as possible.preferably within 12 hours and not
later than 48 hours. HBIG should be given at a contralateral site
at the same time.
(3) Accidental inoculation or contamination of the eye, mouth
or skin with blood or other bodily fluids from a known HBsAg
positive individual. Those who have already been vaccinated
should be given a booster dose.
(4) Sexual Consorts, (and in some circumstances a family
contact judged to be at a high risk ) of individuals suffering
from acute hepatitis B, and who are seen within one week of
jaundice in the contact.
HBV and Hepatocellular Carcinoma
Hepatocellular carcinoma (HCC) is one of the 10 most common
cancers in the world, with over 250000 new cases per year. HCC is
more common in males than females and the incidence of the tumour
reaches a peak in 30 - 50 age group. The geographical areas with
a high incidence of HCC coincides with areas with a high
incidence of hepatitis B. Furthermore, most patients with HCC are
HBsAg +ve and have high titres of anti-HBc. HBV infection in
these areas usually occurs at a young age - in China and S.E.Asia
the virus is usually acquired perinatally from a carrier mother
whereas in Africa, the infection tends to be acquired in early
childhood through horizontal spread of the virus. Therefore there
is a long interval before the development of HCC following the
initial virus infection. The relative risk of developing HCC in a
HBV carrier varies considerably between different ethnic groups,
between 40 to 300 fold compared to the normal population. The
data on relative risk needs to be reassessed in most studies
because many of the subjects had dual hepatitis B and hepatitis C
infection.
Analysis by DNA-DNA hybridization reveals integrated HBV DNA
in approximately 80% of HCC from HBsAg carriers. It is possible
that more sensitive technique such as PCR may lead to a higher
rate of detection. There is also an animal model available in the
form of hepatomas in woodchucks infected with the woodchuck
hepatitis virus.
Mechanisms_for_oncogenesis
primary HCC usually develops in a liver which is affected by
chronic hepatitis or cirrhosis and it has been suggested that
cirrhosis is the main driving force behind the development of
HCC. However, it is clear that HCC is much more likely to develop
in an HBV-infected cirrhotic liver than one that is not
cirrhotic. Furthermore, HCC can develop in the livers of HBV
carriers without an intermediate cirrhotic stage. The finding of
integrated viral DNA suggests a direct role for the virus in
oncogenesis. In the 20% of cases where HBV DNA is not detected, a
'hit and run' mechanism may be involved. Integrated DNA is
commonly found in the liver cells of HBV carriers, especially in
e -ve carriers. integrated viral DNA may be detected in both e
+ve and e -ve carriers, the time of integration is around the
time of seroconversion of the e antigen. The mechanisms involved
in HBV induced oncogenesis is still uncertain. It may take the
form along the following lines ;-
Promoter insertion - This envisages the insertion of a
viral promoter in front of a cellular oncogene leading to the
transcription of the c-onc. There is little experimental
support of this hypothesis.
Introduction of a viral coded oncogene - there is no
evidence that HBV contain such a gene and it has not been
possible to transform cells in vitro using the virus or viral
DNA.
(Insertions mutagenesis - The integration of the viral
genome results in the introduction of an enhancer sequence or
a promoter sequence or may disrupt a cellular gene. Again
there has been very little experimental evidence.
(Transcriptional activation - the X gene of HBV
contains a transcriptional activator. This gene may play a
role in disrupting the normal transcriptional control of the
cell.
Hepatitis B Variants
Pre-core mutants
The core/pre-core gene can be translated into either HBcAg or
HBeAg. HBeAg is found in the serum and the surface of hepatocytes
but not as part of the viral particles. Translation of the
pre-core region is only necessary for the production of HBeAg.
HBeAg and HBeAg and HBcAg shares antigenic epitopes. However,
because of differences in the secondary structures of HBeAg and
HBcAg, there are also unique antigenic determinants. Chronic
carriers of HBV eventually lose HBeAg and seroconvert to
anti-HBe. After an exacerbation of hepatitis, the liver disease
becomes quiescent. However, some patients have progressive
disease characterised by high concentrations of HBV DNA in serum,
and mutant viruses are selected which can no longer produce
HBeAg. This process occurs commonly. The most frequent mutation
results in a premature stop codon in the pre-core region,
terminating the translation of HBeAg. However, the translation of
the core protein is not affected.
It is believed that hepatitis is due to the immune-mediated
killing of hepatocytes and that HBeAg is an important target.
Those hepatocytes that are infected with the pre-core variants
will survive the process. This strategy is obviously a potent
mechanism to prolong infection. Since HBeAg shares antigenic
epitopes with HBcAg, it is postulated that HBeAg plays an
important role in inducing immunological tolerance to HBcAg. By
this mechanism, infants become chronic carriers without liver
damage. However, eventually, the tolerogenic effect will be lost
and an immune response will be mounted against HBeAg, resulting
in hepatitis and the selection of pre-core mutants.
The pre-core mutant form is also associated with fulminant
acute hepatitis. If an anti-HBe positive mother infects her
infant, the child is likely to have more severe acute hepatitis
than if the mother were HBeAg positive. The mutant had been
associated with an outbreak of fulminant hepatitis. These
patients are HBeAg negative. The fulminant course may also relate
to the proposed tolerising effect of HBeAG. In those patients
infected from the beginning with a pre-core mutant, the lack of
HBeAg would allow the immune system to destroy hepatocytes in an
unrestricted fashion. An alternative explanation is that the
patient may be genetically predisposed to mount a very active
immune response against the HBeAg producing strain, leading to
extensive hepatitis and the rapid selection of the mutant.
Fulminant hepatitis does not seem to be as widespread as would be
predicted in those countries in which the anti-HBe positive form
of chronic hepatitis is common. Perhaps this mutant is not as
transmissible as the HBeAg positive strain.
Surface_mutants
Most cases of mutants arise in the "a"
determinant of HBsAg. Current vaccines are not thought to be able
to protect against infection by this mutant. In addition, there
may be problems with the detection of these variants by the
current immunoassays