For years, the nature of the agent(s) responsible for
parenterally transmitted non-A, non-B hepatitis remained
enigmatic, though the involvement of a virus appeared likely.
Chimpanzee transmission studies carried out by Ian Bradley of the
CDC Atlanta made available a pool of serum with a high titre of
antibodies against an agent responsible for parenterally
transmitted non-A, non-B hepatitis. The putative virus was
pelleted from the serum and, because it was not known whether the
genome was DNA or RNA, a denaturation step was included prior to
the synthesis of cDNA so that either DNA or RNA can serve as a
template. The cDNA was then inserted into lambda gt11 expression
vector. Serum from a patient with non-A, non-B hepatitis was used
to screen the cDNA library for clones which may be expressing the
fusion protein antigen. Over 1 million clones were screened. This
approach led to the detection of a clone (5-1-1) which was
recognized by the sera of several infected patients. This clone
was used as a probe to detect a larger overlapping clone in the
same library. It was possible to demonstrate that these sequences
hybridized to a positive-sense RNA molecule of around 100,000
nucleotides which was present in the liver of infected
chimpanzees. Using gene walking techniques, additional clones
with virus sequences in the library were identified and in due
course, the complete nucleotide sequence of the virus became
available. The organization of the genome closely resembled those
of enveloped RNA viruses. To date, the virus has yet to be
convincingly visualized by EM.
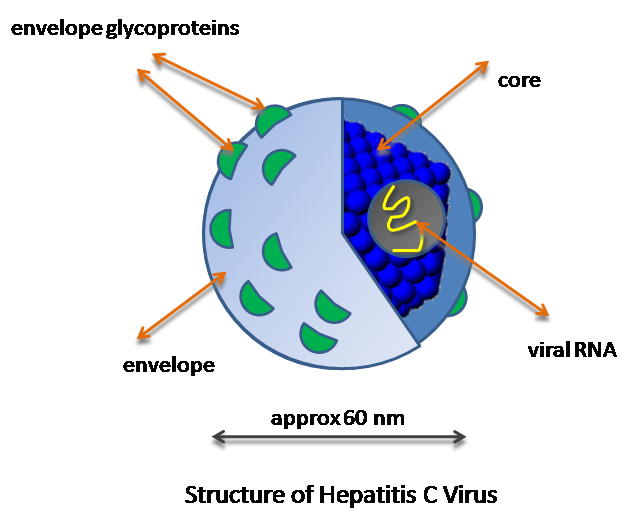
Properties
Genome resembled that of a flavivirus
positive stranded RNA genome of around 10,000 bases
1 single reading frame, structural genes at the 5' end, the
non-structural genes at the 3' end.
enveloped virus, virion thought to 30-60nm in diameter
morphological structure remains unknown
Epidemiology
In America, since HBsAg screening was introduced, the
incidence of post-transfusion hepatitis has a declined, but a
significant number of cases remained. At least 95% of
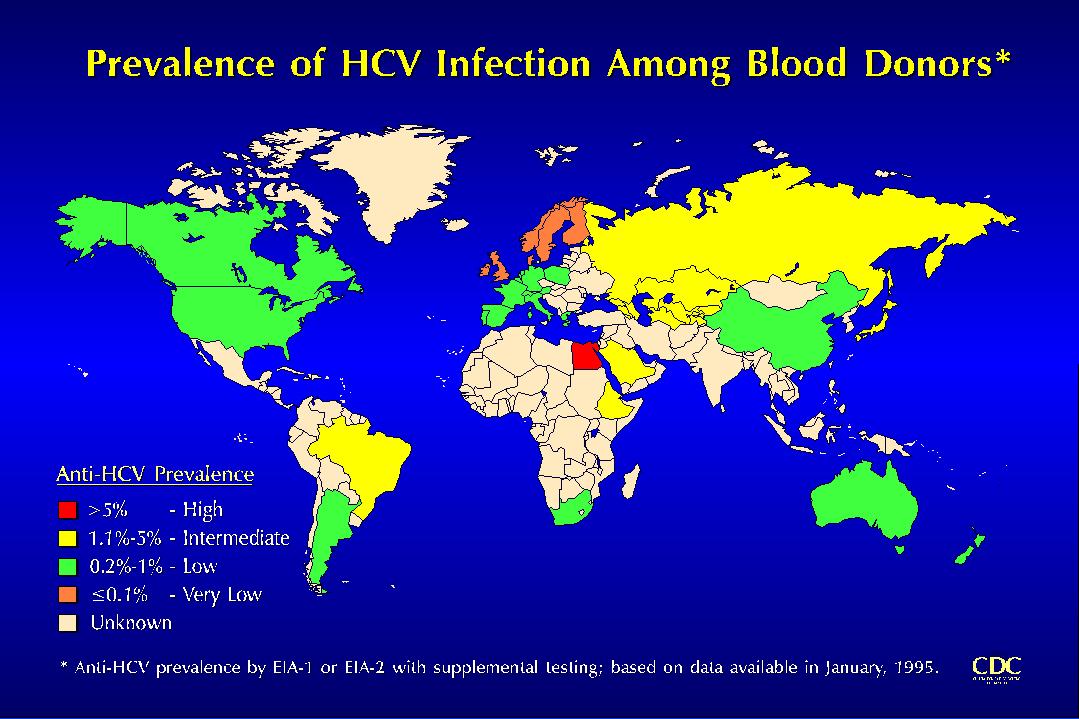
post-transfusion hepatitis was caused by non-A non-B. Worldwide,
there are thought to be 100 million carriers of hepatitis C. It
is particularly prevalent in Japan, where it is thought to be
responsible for the majority of cases of hepatocellular
carcinoma. There are 175,000 new cases of hepatitis C in the US
per year. In the US, NANBH infection is more common than HBV
infection amongst IVDA and those given blood transfusions. NANBH
is usually transmitted parenterally. Sexual transmission can
occur albeit considerable less efficient for HBV. There were
recent reports of vertical infection.
The highest HCV antibody prevalence is found in haemophiliac
patients who have received untreated blood or blood products
where up to 85% of such patients in the UK have antibodies. A
large proportion of cases occur in people with no known risk
factors. The evidence for and against sexual spread is confusing.
It is noteworthy though that 20% of non-drug using female
partners of IV drug users with hepatitis C are positive for
anti-HCV. In general, the mode of HCV transmission is similar to
HBV.
Health care workers experiencing needlestick injuries are also
at risk of acquiring HCV infection. In one study, 3% of health
workers with a needlestick exposure in which the source patient
was anti-HCV positive converted to anti-HCV. Accumulating
evidence indicates that HCV is transmitted from mother to infant;
however the actual risk is unknown. Anti-HCV seroconversion has
only been rarely documented among infants born to anti-HCV
positive mothers unless their mothers were also infected with
HIV. However, in studies using PCR, HCV transmission apparently
occurred without anti-HCV seroconversion.
In common with other RNA viruses, wide genetic variation of
hepatitis C exist in nature. On the basis of phylogenetic
analysis, HCV has been classified into six major genotypes (types
1 to 6) of which four (types 1 to 4) contain several more closely
related subtypes (e.g. a, b and c). In West-ern Europe and the
USA, the predominant geno-types are la, lb, 2b and 3a, with some
variation in frequency. In Japan and Taiwan types lb, 2a and 2b
are seen most frequently. Elsewhere in Asia, genotype 3 is the
most common, and genotype 4 is found frequently in the Middle
East and Africa. Type 5 is mainly found in Southern Africa and
type 6 in SE Asia. There is increasing evidence demonstrating a
link between HCV genotype and disease severity and
re-sponsiveness to interferon therapy. Genotype lb was found
significantly more often in cases of severe liver disease such as
cirrhosis and hepatocellular carcinoma. It was also associated
with a longer disease duration and a higher level of viraemia
than other genotypes. Individuals infected with genotype 1b are
less likely to respond to interferon therapy
Pathogenesis
Each clinical form of viral hepatitis with HBV can also occur
with HCV. Acute disease may lead to recovery, fulminant
hepatitis, relapsing hepatitis with intervening periods of normal
liver function, inapparent chronic infection, chronic active
hepatitis and cirrhosis have been documented. The incubation
period lies between that of HAV and HBV. HCV infection is
particularly associated with high ALT levels and it was suggested
that ALT levels could be used as surrogate marker for the
screening of NANBH before the availability of a test for
anti-HCV.
Chronic Infection - It is thought chronic infection
occurs in 50- 75% of all patients infected with HCV, in contrast
to 10% for adults infected with HBV. In a cohort study where
patients with HCV chronic disease had been followed up for 10
years, 20% have cirrhosis, 30% made improvements, 45% remained
stable, 25% have shown progression (including the development of
cirrhosis).
Association with hepatocellular carcinoma - Several
recent studies have established a strong association between HCV
and hepatocellular carcinoma. anti-HCV antibodies, in the absence
of HBV markers, were detected in 44.5% of HCC patients in Spain,
43% in Japan, 16% in Italy, 7% in South Africa. Since HBV
carriers often have chronic HCV infection, it is conceivable that
the 2 viruses may act together to cause HCC and epidemiological
data linking HBV to HCC may require reassessment in terms of the
magnitude of the risk involved with the availability of testing
for chronic HCV infection. HCV may prove to be as important as
HBV in the causation of hepatocellular carcinoma worldwide. It
has recently been suggested that the risk of developing HCC is
approximately 5% year in cirrhotic patients with chronic
hepatitis C; this is greater than the risk from hepatitis B.
In chimpanzees and to a lesser extent in humans, cytoplasmic
tubules (cylindrical confronting cisternae) are regularly seen
under EM. The nature of these structures are unknown in
particular to the part they may play in HCV replication. In HCV
hepatitis, direct cytopathic damage to the hepatocytes is thought
to be the mechanism of pathogenesis, in contrast to the
immunopathological mechanisms in HBV.
HBV
HCV
Symptomatic
50
10-35
Chronicity
10-15
50-75
Hepatocyte injury CMI direct CPE
In general, hepatitis C is a slower disease than hepatitis B.
It takes 10 years to develop chronic hepatitis, 20 years to
develop cirrhosis, and 30 years to develop hepatocellular
carcinoma. There are certain nonhepatic disorders which are
sometimes associated with chronic hepatitis C infection. eg.
mixed cryoglobulinaemia, membranoproliferative
glomerulonephritis, Sjogren's syndrome, sporadic porphyria
cutanea tarda, and lichen planus.
Laboratory Diagnosis
1. Serology - the first generation ELISA kits relied on
a fusion protein antigen produced from a original 5-1-1 clone
with a few adjoining clones. The antigen was denoted as the C100
antigen. The problem with the first generation kits was that the
antigen used was non-structural and thus may not pick up all
cases of HCV. Furthermore, antibodies against this antigen could
not be detected until 15 weeks after the onset of hepatitis.
Therefore, HCV infection cannot be excluded in those whose serum
is antibody-negative up to 6 months after the onset of symptoms.
The first generation kits had also been demonstrated to have a
poor specificity. Second and third generation assays are now used
for serological diagnosis. Second generation assays incorporate
C22 core antigen as well as NS4 (C-100-3) and NS3 antigens. The
newer third generation assays incorporate NS5 as an additional
antigen. However this increase in sensitivity is offset by a
slight decrease in specificity. They reduce the "diagnostic
window" down to 4 weeks after initial infection.
Recombinant Immunoblot assays (RIBA) were developed by Ortho
whereby nitrocellulose strips were coated with discrete bands of
E. coli and yeast cloned antigens. It is thought that
this test carried a much higher specificity with equal
sensitivity. Another method to increase sensitivity was to use
"blocking tests". Sera positive for anti-HCV were
blocked by C-100-3 antigen. Inability to be blocked is
interpreted as non-specificity. Recombinant antigens are being
developed based on structural proteins which should lead to
serological tests with higher sensitivities. Also it is feasible
that antibodies to these antigens may appear earlier and thus
diagnosis of acute infection may become possible.
2. Detection of HCV-RNA - Real time quatitative PCR tests had been
developed where the level of HCV viraemia is roughly quantified
and thus infectivity of the blood. A 5' conserved non-coding
region had been identified. PCR has enormous potential value in
support of the anti-HCV ELISA and in the study of HCV. It can be
used to diagnose acute infection as HCV viraemia occurs well
before the development of anti-HCV antibodies. Evidence provided
by PCR for fluctuated level of infectivity in certain individuals
may play an important role in the consideration of infectivity of
seropositive donors. RIBA-2 positivity appears to correlate well
with PCR positivity. A branched DNA assay has also been developed
for the detection of HCV-RNA. Quantitation of HCV-RNA is important in monitoring
the response to antiviral therapy.
3. Hepatitis C Antigen - Recent reports described the
identification of hepatitis C antigen (HCAg) in hepatocytes of
patients suffering from chronic HCV infection using a FITC
polyclonal IgG obtained from patients with hepatitis C. A test
for hepatitis C antigen in serum is being developed for the
detection of HCV viraemia, rather like PCR.
4. HCV Genotype - There are six known genotypes and
more than 50 subtypes of hepatitis C. Determining the HCV genotype is useful in
epidemiological research and also in making recommendations regarding therapy.
Patients with genotypes 2 and 3 are two to three times more likely to respond to
interferon-based therapy than patients with genotype 1. Furthermore, when using
combination therapy, the recommended dose and duration of treatment depend on
the genotype. For patients with genotypes 2 and 3, a 24-week course of
combination treatment using peginterferon and 800 milligrams (mg) of ribavirin
daily is adequate, whereas for patients with genotype 1, a 48-week course and
full dose of ribavirin (1,000 to 1,200 mg daily) is recommended. For these
reasons, testing for HCV genotype is clinically important.
Treatment
Early studies indicate that interferon and ribavirin are
effective of cases of acute and chronic hepatitis C. A
combination of interferon and ribavirin may be useful. There is
more experience in the use of interferon for the treatment of
hepatitis C. The current recommendation is that interferon
treatment may be considered in those with chronic active
hepatitis who are at risk of progression to cirrhosis and HCC.
The recommended regimen is 3 MU tds sc or im for 6 months. The
response rate is around 50%. However, approximately 50% of
responders relapse upon cessation of treatment. At present, it is
not clear what factors predict response to interferon therapy.
There is some data to suggest that older patients and those with
established cirrhosis respond less well. There is also growing
evidence that the genotype of the infecting HCV determines the
response to IFN. Type 1, in particular is associated with poor
response to IFN. Therefore, a 48 week course of therapy is recommended for these
patients instead of 24 weeks for genotypes 2 and 3. A newer preparation of
interferon (peginterferon) is now available that allows for weekly injections.
However, it must be given for 48 weeks irrespective of the genotype.
Protease inhibitors have emerged as a third feature of
combination therapy. The first protease inhibitors licensed were boceprevir (Victrelis)
and telaprevir. However they are now superseded by more effective options.
Simeprevir (Olysio) was licensed in 2013 and is now recommended as part of
combination therapy. More recently, HCV NS5B polymerase inhibitor sofosbuvir (Sovaldi)
has emerged as an important component of currently recommended regimens. In
November 2014, the FDA approved an all oral regimen of simeprevir plus
sofosbuvir for treatment-naïve or treatment-experienced patients. On December
19, 2014, the FDA approved the combination of ombitasvir/paritaprevir/ritonavir
and dasabuvir (Viekira Pak ) for the treatment of genotype 1 chronic hepatitis C
infection in adults, including patients with compensated cirrhosis. In the
Viekira Pak, ombitasvir, paritaprevir, and ritonavir are combined as a
fixed-dose tablet and the dasabuvir is a separate tablet. This all oral
treatment can be given with or without ribavirin. In Aug 2017, the FDA gave
approval for glecaprevir and pibrentasvir (Mavyret, AbbVie Inc) for treatment of
hepatitis C. The drug is indicated to treat adult patients with chronic
hepatitis C (HCV) genotypes 1-6 without cirrhosis or with mild cirrhosis,
including patients with moderate-to-severe kidney disease and those who are on
dialysis.
It also appears that the level of viraemia at
the commencement of treatment predicts the response. Most
responders will have significant reduction of SGPT level within 2
months of interferon therapy. One may try a higher dose such as 5
or 10 MU in non-responders although it is not certain whether the
higher doses work. At present, it is not clear what factors
predict relapse after treatment. For those who relapse after
treatment, they may be offered a second course and then put on
maintenance therapy for 6 to 12 months. It is important to monitor the
response to antiviral therapy virologically during the treatment period.
Commercial quantitative PCR and bDNA assays are usually used for this purpose.
Prevention
The introduction of HCV screening in the blood transfusion
service should reduce significantly the number of cases of post-
transfusion hepatitis C. However, the extra cost is high as the
current screening ELISA is 5 times more expensive than the
anti-HIV screen test. Inactivation procedures should eliminate
the risk of HCV spread via blood products. However, the above
measures would only contribute to the prevention of a small
proportion of cases of hepatitis C. Therefore, further preventive
measures would depend on a better understanding of the
epidemiology of hepatitis C infection. The efficacy of
immunoglobulin for pre- or post-exposure prophylaxis is
controversial. Vaccine development is going on and animal trails are being
carried out.