Influenza Viruses
Influenza is commonly seen in local outbreaks or epidemics throughout the world. Epidemics may appear at any time but are usually concentrated in months of high humidity. They occur explosively with little or no warning. The number of people affected can vary from a few hundred to hundreds of thousands. Epidemics may be short-lived, lasting days or weeks but larger epidemics may last for months. Although influenza is a mild disease in most individuals, it is life threatening to elderly or debilitated individuals. Epidemics are responsible for large losses in productivity. The WHO commissioned an international network of communicating laboratories to monitor the antigenic changes in the infecting viruses and the spread of infection.
A. Properties
Belongs to the genus orthomyxovirus in the family of Orthomyxoviridae. ssRNA enveloped viruses with a helical symmetry. Enveloped particles 80-120nm in diameter.
The RNA is closely associated with the nucleoprotein (NP) to form a helical structure.
The genome is segmented, with 8 RNA fragments (7 for influenza C)
There are 4 antigens present, the haemagglutinin (HA), neuraminidase (NA), nucleocapsid (NA), the matrix (M) and the nucleocapsid proteins.
The NP is a type-specific antigen which occurs in 3 forms, A, B and C, which provides the basis for the classification of human influenza viruses. The matrix protein (M protein) surrounds the nucleocapsid and makes up 35-45% of the particle mass.
2 surface glycoproteins are seen on the surface as rod-shaped projections. The haemagglutinin (HA) is made up of 2 subunits, HA1 and HA2. HA mediates the attachment of the virus to the cellular receptor. Neuraminidase molecules are present in lesser quantities in the envelope.
Electronmicrograph of influenza virus particles. (Courtesy of Linda M. Stannard, University of Cape Town)
Virus Classification - On the basis of their nucleocapsid and M protein antigens, the influenza viruses are divided into 3 distinct immunological types. (A, B, and C) Influenza A viruses also occur in pigs, birds, and horses. However, only man is infected by influenza B and C. The antigenic differences of the haemagglutinin and the neuraminidase antigens of influenza A viruses provide the basis of their classification into subtypes. eg. A/Hong Kong/1/68 (H3N2) signifies an influenza A virus isolated from a patient in 1968, and of subtype H3N2.
The explosive nature of epidemic influenza and the specific clinical features of this disease have given reliable epidemiological records of this infection since the beginning of the nineteenth century. Several epidemics were recorded during the nineteenth century but the first pandemic was not accurately recorded until 1889-92. A second pandemic, probably originating in Europe, occurred in 1918-19, and is known as Spanish Influenza. It is responsible for 20-25 million deaths, principally in young adults. It was suggested that this strain had unusual virulence. Alternatively, the large numbers of deaths may be due to the debilitating conditions as a result of the First World War. In fact, the number of deaths recorded may only be a fraction of the true number.
Pandemics continued to occur regularly after the Spanish influenza, in 1932-33, 1947-48, 1957, 1968, and 2009 These latter pandemics resembled the pandemic of 1890, affecting millions of people with a mild URTI and a small number of deaths. The H1N1 (swine) viruses probably appeared in 1918 and continued to circulate until 1957, at which time they were supplanted by the H2N2 (Asian) viruses. The H2N2 viruses were prevalent until 1968, when H3N2 (Hong Kong) strains appeared. The H1N1 virus reappeared in 1977 and did not replace the H3N2 subtype and both subtypes continued to cocirculate. In 2009, a novel strain of H1N1 appeared that was distinct from the prevailing H1N1 strain that appeared in 1997. From its initial detection in Mexico in April 2009, it rapidly spread to the U.S. and around the world and was declared a pandemic by the WHO in June 2009.
1. Antigenic Shift
The recorded patterns of influenza A infection contain 2 phenomena; the first being the almost identical annual epidemics which occur in most countries, and the second are the extensive pandemics which occur approximately every 10 - 12 years. Analysis of virus isolates since 1933 showed that viruses isolated in the years 1933-46, 1947-56, 1957-67, and from 1968 onwards demonstrated wide variation. Virus specific sera raised from ferrets did not cross react in HAI tests. It is apparent that pandemics are due to the appearance of new influenza A subtypes against which the population has no immunity. This phenomenon is known as antigenic shift. As immunity to the new subtype builds up, further epidemics are more limited. The appearance of a new influenza virus subtype is paralleled by the disappearance of the old subtype (an exception occurred in recent times, when 2 virus subtypes have circulated concurrently) The HA antigen is always involved in antigenic shift as it is responsible for eliciting virus-neutralizing antibodies. The neuraminidase may be affected as well. The origin of antigenic shift has been a subject of intensive research but has yet to be resolved. There are 3 theories as to how antigenic shift arise and they are not mutally exclusive: there is evidence for all 3 theories in past pandemics
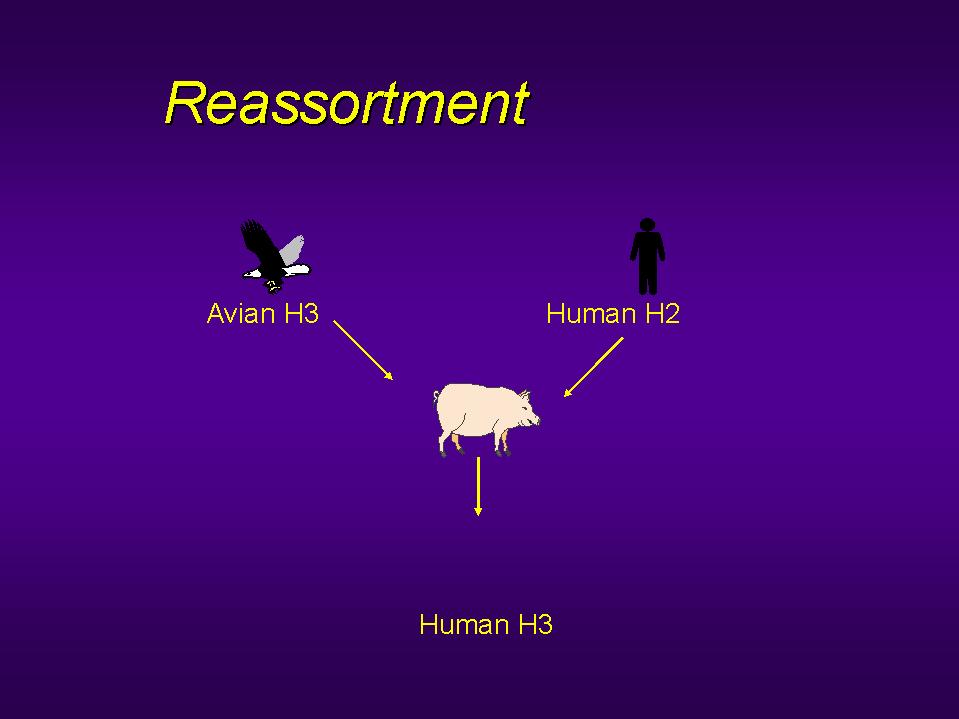
Reassortment - the most widely held view is that
the new virus subtypes are reassortant viruses resulting
from double infection, so that that 8 RNA segments of
each strain reassortment with each other, producing a new
virus. As the appearance of the new subtype is paralleled
by the disappearance of the old subtype, it is unlikely
that the dual infection was by 2 human influenza A
subtypes. However, influenza A viruses infect other
species of animals, such as horses and birds. It was
postulated that dual infection with human and animal or
bird viruses could result in the production of a
reassortant virus. Indeed, such reassortant viruses have
been produced in the laboratory from human and animal
parents. Influenza A viruses can cross species barrier.
The pig is postulated as the most likely "mixing
vessel" as it can be infected by both human and
avian viruses. Such an event is most likely in occur in
SE Asia, in particular China, where humans and animals
live in close proximity. There is no pretty good evidence
that such an event occurred in 1947 when H1N1 was
replaced by H2N2, and in 1968 when H2N2 was replaced by
H3N2. The H1N1 strain that caused the 2009 pandemic was thought to be a
triple reassortant between human, bird, N. American and Eurasian pig
influenza viruses. Influenza B viruses do not occur in animals and do
not exhibit antigenic shift. This has been put forward as
indirect evidence for recombination as the mechanism for
the emergence of new influenza A subtypes.
Recirculation of existing subtypes - It has also
been suggested that there are a limited number of
influenza A subtypes which are recycled in the human
population. Evidence for this theory comes from
seroepidemiological studies of antibody to influenza
viruses in sera taken at different times from subjects of
different ages. Antibody to a human influenza A subtype
was often found in the sera of elderly persons taken
years before the appearance the appearance of the same
subtype as a cause of pandemic infection. It was
suggested that all influenza A subtypes exist in nature,
and emerge when the antibody status of the population has
fallen to levels which allow pandemic infection: a cycle
of approximately 70 years. However, the evidence
supporting this theory is very fragile. In 1977 H1N1
reappeared which was very similar to the strain which
circulated before 1957. It was widely believed that it
may have escaped from a laboratory. As a sizable
proportion of the population had already been exposed to
the H1N1 virus before 1957, it did not cause a pandemic.
Gradual adaptation of animal viruses to human transmission - A third mechanism for antigenic shift is the gradual adaptation of avian viruses to human transmission. There is now evidence that this might have happened in the 1918 pandemic: that the pandemic virus was directly descended from an avian ancestor.
Reassortment of human H2 with avian H3 virus: there is strong evidence that this occurred with the emergence of the H3N2 pandemic virus in 1968.
2. Antigenic Drift
In addition to the large pandemics due to antigenic shifts for influenza A viruses seen every 10 - 12 years, smaller epidemics occur regularly in the intervening years. The viruses isolated from such epidemics showed strain differences when compared in the HAI tests ie. although the viruses belong to the same subtype, they do not cross react completely. These lesser antigenic changes are known as antigenic drift. Antigenic drift is thought to arise through natural mutation, and selection of new strains takes place by antibody pressure in an immune or partially immune population. Epidemics due to new virus strains arising due to antigenic drift is not as great as for those showing antigenic shift, since partial immunity is present in persons with cross- reacting antibody induced by previous infection.
Virus infection is spread via respiratory droplets. The virus
particles binds to cells of the respiratory epithelium which are
rich in viral receptors. Neuraminidase present on the virus
particles aid the infectious process by releasing virus particles
which have been bound by the mucous present on the surface of
epithelial cells. Because of the generalized symptoms present,
viraemic spread form the respiratory tract has been suspected,
although there is no conclusive evidence.
Following a typical incubation period of 48 hours, the typical symptoms of influenza appears. The onset is abrupt with a marked fever, headache, photophobia, shivering, a dry cough, malaise, myalgia, and a dry tickling throat. The fever is continuous and lasts around 3 days. Influenza B infection is similar to influenza A, but infection with influenza C is usually subclinical or very mild in nature.
Complications
1. Tracheobronchitis and bronchiolitis - A small
proportion of patients develop more sever respiratory
symptoms where rales and rhonchi are heard but the chest
is radiologically clear. These symptoms are more commonly
seen in the elderly and patients with COAD.
2. Pneumonia - primary viral pneumonia or a
secondary bacterial pneumonia may develop. Primary viral
pneumonia is relatively uncommon, but cases have been
demonstrated in many influenza epidemics. It may occur in
previously young and healthy persons, but are commonly
associated with patients with preexisting cadiovascular
disease such as Rheumatic fever. Secondary bacterial
pneumonia is more common than primary viral pneumonia. It
was speculated that the high incidence of deaths in young
people during the Spanish influenza pandemics of
1917-1918 may have been due to secondary bacterial
pneumonia in a population generally debilitated by the
effects the WWI.
Secondary bacterial pneumonia - usually
occurs late in the course of disease, after a period of
improvement has been observed for the acute disease. The
symptoms and signs are that of a typical bacterial
pneumonia. S. aureus is most commonly involved
although S. pneumoniae and H. influenzae
may be found. There appears to be a good reason why S.
aureus is so commonly found in cases of secondary
bacterial pneumonia. Infection of cells by influenza A
requires cleavage of the virus haemagglutinin by
proteases, and some strains of S. aureus produces
such enzymes. Thus S. aureus and influenza may
promote infection by the other. Influenza A by damage to
the healthy respiratory epithelium.
Myositis and myoglobinuria - In addition to
myalgia, which is characteristic of acute influenza
infection, clinical myositis and myoglobinuria may occur.
Reye's syndrome - Reye's syndrome is characterized
by encephalopathy and fatty liver degeneration. The
disease has a 50% mortality amongst hospitalized cases
and had been associated with several viruses; such as
influenza A and B, Coxsackie B5, echovirus, HSV, VZV, CMV
and adenovirus.
Other complications - influenza infection have
been implicated in acute viral encephalitis and
Guillain-Barre syndrome. Influenza A was also associated
with the cot death syndrome.
During epidemics, a presumptive diagnosis can be made on the basis of the clinical symptoms. However, influenza A and B can co-circulate, and mixed infections of influenza and other viruses have been reported. Isolated cases of suspected influenza should be investigated for these may represent the first cases of an impending epidemic.
Rapid Diagnosis - Nasopharyngeal aspirates are the specimens of choice as they are the most sensitive. However, throat and nasal swabs are more commonly used given the difficulties involved in taking nasopharyngeal aspirates.
Cells from pathological specimens may be examined for the presence of influenza A and B antigens by indirect immunofluorescence. Although many workers are convinced of the value of this technique, others have been disappointed with the specificity of the antisera and the level of background fluorescence that makes the test difficult to interpret. Type specific sera are available that could differentiate between H3 and H1 viruses. However, they could not differentiate between the seasonal H1N1 and the 2009 pandemic H1N1.
EIA tests for the detection of influenza A viral antigens are available that are easier to interpret than immunofluorescence since whole cells are not required. Commercially available tests could not differentiate between H3N3 and H1N1 influenza.
RT-PCR assays for the detection of influenza RNA are available that provides the greatest sensitivity and specificity. Moreover, the PCR product can be sequenced for strain identification and epidemiological investigation. RT-PCR assays were the only rapid assays available for the identification of the 2009 pandemic H1N1 virus and proved invaluable during the pandemic. However, RT-PCR assays are very expensive and the test had to be rationed once the number of suspected cases become overwhelming.
Virus Isolation - Throat swabs, NPA and nasal
washings may be used for virus isolation. It is reported
that nasal washings are the best specimens for virus
isolation. The specimen may be inoculated in embryonated
eggs or tissue culture. 10-12 day embryonated eggs are
used for virus isolation. The specimen is inoculated into
the amniotic cavity. The virus replicates in the cells of
the amniotic membrane and large quantities are released
back into the amniotic fluid. After 2-3 days incubation,
virus in the amniotic fluid can be detected by adding
aliquots of harvested amniotic fluid to chick, guinea
pig, or human erythrocytes. Pathological specimens can be
inoculated on to tissue cultures of kidney, chicks or a
variety of other species. Rhesus monkey cells are the
most sensitive. Although no CPE is produced, newly
produced virus can be recognized by haemadsorption using
the cells in the tissue culture, and haemagglutination
using the culture medium which contains free virus
particles. Influenza B virus and occasionally influenza A
will produce a CPE in MDCK cells. Influenza viruses
isolated from embryonated eggs or tissue culture can be
identified by serological or molecular methods. Influenza
viruses can be recognized as A, B, or C types by the use
of complement fixation tests against the soluble antigen.
(A soluble antigen is found for all influenza A, B or C
type virus but antibody against one type does not cross
react with the soluble antigen of the other. The further
classification of influenza isolates into subtypes and
strains is a highly specialized responsibility of the WHO
reference laboratories. The HA type is identified by HAI
tests, the NA type is also identified.
Serology - Virus cannot be isolated from all cases of suspected infection. More commonly, the diagnosis is made retrospectively by the demonstration of a rise in serum antibody to the infecting virus. CFT is the most common method used using the type specific soluble antigen. However, the CF test is thought to have a low specificity. A more specific test is the HAI test. Infection by influenza viruses results in a rise in serum antibody titre, but the requirement for a 4-fold or greater rise in titre of HI of CF antibody reflects the inaccuracy of these tests for detecting smaller increases in antibody. A more precise method for measuring antibody is by SRH. SRH is more sensitive than CF or HAI tests and has a greater degree of precision. A 50% increase in zone area represents a rise in antibody and is evidence of recent infection. Sera do not have to be pretreated to remove non-specific inhibitors which plaque the HAI test. SRH may well replace CF and HAI tests in diagnostic laboratory in future.
Influenza epidemics are responsible for massive disruption to industry, and for a significant number of deaths, particularly in the elderly and the very young. At present, treatment of influenza is entirely symptomatic. Salicylates should be avoided in children because of the link with Reye's syndrome. Neuraminidase inhibitors, in particular Oseltamivir have replaced Amantidine as the anti-viral drug of choice in the treatment of influenza infections.
Oseltamivir (Tamiflu) - the rational
approach to drug design has led to the design of several potent inhibitors
of influenza neuraminidase. Oseltamivir is now the drug of choice for the
treatment of influenza. Unlike zanamivir, it can be
given orally. Like zanamivir, it had been shown to be
effective and devoid of significant side effects in
clinical trials. It is approved by the FDA for use as
treatment for influenza A and B in persons 18 years or
older. It is also approved for prophylaxis in persons 13
years or older. Its lack of side effects would make
particularly attractive in a family setting although its
higher cost compared to amantidine and rimantidine should
be taken into account. It is recommended to be given within 48 hours of
the onset of symptoms. Mutations conferring resistance are single amino acid
residue substitutions (His274Tyr) in the neuraminidase enzyme. The
resistance to different types varies enormously year to year. H3N2 strains
were mainly sensitive whereas seasonal H1N1 were almost totally resistant.
More than 98% of the 2009 pandemic influenza H1N1 tested were sensitive.
Zanamivir - Zanamivir was the
first neuraminidase inhibitor available for clinical use
and is effective against both influenza A and B. Because
of its poor bioavailability, zanamivir must be
administered by inhalation. Zanamivir had been shown to
be effective and devoid of significant side effects in
clinical trials. It is now approved by the FDA for use as
treatment for influenza A and B in persons 12 years or
older but not for prophylaxis. Because it cannot be given orally, it
popularity has been eclipsed by oseltamivir.
Peramivir (Rapivab) - Peramivir is another
neuraminidase inhibitor licensed for clinical use. It is approved for IV use
and has been reported to be effective in serious infections.
Amantidine - this compound inhibit the growth of
influenza viruses in cell culture and in experimental
animals. Amantidine is only effective against influenza
A, and some naturally occurring strains of influenza A
are resistant to it. The mechanism of action of
amantadine is not known. It is thought to act at the
level of virus uncoating. The compound has been shown to
have both therapeutic and prophylactic effects.
Amantidine significantly reduced the duration of fever
(51 hours as opposed to 74 hours) and illness. The
compound also conferred 70% protection against influenza
A when given prophylactically. Amantidine can
occasionally induce mild neurological symptoms such as
insomnia, loss of concentration and mental
disorientation. However, these symptoms quickly developed
in susceptible individuals and cease when treatment is
stopped. The therapeutic and prophylactic activity of
amantidine is now generally accepted and numerous
analogues of this compound have been prepared.
Rimantadine is not as effective as amantadine but is less
toxic. Prophylaxis with 200mg of amantadine per day for 5
to 6 weeks or for the duration of the influenza A
outbreak is not recommended for all persons. However,
elderly persons with chronic underlying disease,
institutionalized persons, staff and patients in
hospital, close contacts of an index case, and patients
who cannot receive influenza A vaccine due to sensitivity
to egg protein may benefit from prophylaxis. Amantadine
can also be used for therapy of uncomplicated influenza A
infections. The recommended dose is 200mg for 5 days.
Rimantadine may be used in place of amantadine for
prophylaxis and the treatment of uncomplicated influenza
A infections.
Rimantidine - this compound is similar
to amantidine but has fewer side effects. It is approved
by the FDA for the treatment and prophylaxis of influenza
A infection in persons one year or older. It should be
used for uncomplicated influenza A infections only since
it is thought to be less effective than amantidine.
Amantadine and rimantadine resistant viruses are readily
generated in the laboratory. Resistance has been linked
to changes in the M2 protein. To date, the emergence of
resistant influenza A has been documented primarily in
young children undergoing therapy with rimantadine. The
resistant viruses had been transmitted and caused
influenza. The universal susceptibility of all types of
naturally occuring influenza A isolated from man and
animals suggests that resistance will be found only in
individuals treated with the drug. The reason for the
natural selection of the susceptible phenotype of
influenza A in nature is not known.
Vaccines against influenza have been around for 50 years. Despite this, the efficacy of influenza vaccines is still questioned, and the ability of vaccines to limit epidemic infection has not been proven.
1. Immunity to Influenza - the results of challenge studies indicated that immunity is induced by the host responses to the virus haemagglutinin (HA) and to neuraminidase (NA). Antibody against HA is the most important component in the protection against influenza viruses. In addition to conferring relative protection against infection, serum HI is reported both to reduce the severity of infection and decrease virus spreading in infected persons. Serum anti-neuraminidase Ab has also been shown to contribute protection against influenza infection. A generally held view is that serum HI antibody is more important in determining immunity than anti-neuraminidase antibody. It is clear that an influenza vaccine must contain both HA and NA antigens in a form which will stimulate the production of neutralizing antibody, local IgA antibody and possibly cellular immunity.
2. Types of vaccine
Whole virus vaccines - whole inactivated virus
vaccines were the first influenza vaccines to be
produced. The currently circulating strain of influenza
is inoculated into embryonated eggs, harvested 2-3 days
later and inactivated. this vaccine confers protection in
60-90% of vaccinees and the protection lasts for 1-5
years, depending on the vaccine strain and the age of the
vaccinee. However, the subsequent infecting virus may
show slow antigenic drift and the vaccine induced
antibody will be less effective in conferring protection
against the new strains.
Split virus vaccines - Because of the high
incidence of reactions seen in vaccinees given whole,
inactivated virus vaccine, attempts have been made to
produce a vaccine which is less reactogenic but
conserving immunogenicity. Split vaccines were prepared
inactivated particles disrupted with detergents. These
vaccines have been shown to induce fewer side effects in
the vaccinees and are just are immunogenic as whole virus
vaccine. Whole virus vaccine should not be used in
children.
Subunit virus vaccines - subunit vaccines have
been prepared which contained only the HA and NA
antigens. These are used in aqueous suspension or may be
absorbed to carriers such as alhydrogel. Volunteers given
subunit vaccines experienced fewer reactions than those
given whole virus vaccines and those given aqueous
vaccine experienced fewer reactions than those given the
absorbed subunit vaccine. therefore, the best vaccines
available at present are the aqueous subunit vaccines,
although some authorities have questioned the
effectiveness of subunit vaccines.
Live attenuated vaccines - there is experimental evidence that immunization with live, attenuated influenza virus vaccines induce a solid immunity than do inactivated vaccines. Normal methods for attenuation, such as repeated passages and temperature adaptation require a long period to complete, and probably too long for the vaccine to become available for immunization against the current influenza strain. To circumvent this problem , already attenuated strains have been mixed with wild-type virus to produce recombinants which contain the RNA fragments which code for wild-type HA and NA, and all the other genetic material form the attenuated strain. These recombinants can be produced relatively quickly. When given intranasally, produced few side effects.
Although research to develop live attenuated vaccines has been pursued for 20 years, basic problems remains particularly in the area of purification. The vaccine must also be shown to be attenuated and safe. It is estimated that if the safeguards are to be satisfied, 2 years would be needed for the development of an attenuated vaccine. This makes their development impractical , since by the time the vaccine virus can be made available, the epidemic strain against which the vaccine has been prepared would have disappeared. For an attenuated vaccine to be a practical proposition, the development time must be down to 6-9 months.
3. Recommendations - At present, no live attenuated vaccine is available for general use. The vaccines that are currently available are produced from virus grown in embryonated eggs. The aqueous subunit vaccine is the most acceptable formulation. These vaccines produce few reactions and confer protection in 60-90% of vaccinees. Vaccination is recommended for the elderly and individuals at risk for severe infection. In addition, key personnel n industry and social and medical services. It is highly debatable whether the vaccine should be given to the general population. Influenza immunization is strongly recommended for adults and children with any of the following:
1. Chronic respiratory disease
2. Chronic heart disease
3. Chronic renal failure
4. Diabetes mellitus and other endocrine disorders
5. Immunosuppresion due to disease or treatment
Immunization is also recommended for residents of nursing
homes and old peoples' homes and other long stay facilities where
rapid spread is likely to follow. Two types of vaccines are
available in the UK; "split virus vaccines", and
"surface antigen" vaccine which contains highly
purified HA and NA antigens prepared from disrupted virus
particles. Both vaccines are suitable for use in children.
4. WHO Influenza Surveillance Program
The WHO has a network of around 110 influenza centres worldwide that regularly submit new influenza isolates to the 4 WHO collaborating centres (US, UK, Japan, Australia) for analysis. The aim is to detect new and potentially dangerous strains of influenza at the earliest moment so that measures can be enacted in the event of a pandemic. The strains used in current influenza vaccines are supplied to the vaccine by the WHO. It is normally a trivalent vaccine: one H3N2, one H1N1 and one influenza A sutype. The sutypes selected are those that are normally the most antigencally diverse strains considered to have to greatest epidemic potential.
The H5N1 avian influenza outbreak in Hong Kong 1997
In the latter half of 1997, an outbreak occurred in Hong Kong
whereby 18 persons were infected by an avian influenza A,
serotype H5N1. Of these 6 died, and 3 others were severely ill.
The source of the outbreak was infected chickens and the outbreak
stopped after all the chickens were slaughtered in the territory.
Large-scale serological studies carried out showed that workers
in the poultry industry were particularly at risk of infection
although none complained of any symptoms. There was evidence of
limited human to human transmission. It was postulated that the
strain of avian influenza involved was unusually virulent; it had
multiple basic amino acids near the cleavage site of the
haemagglutinin protein, which as a result may render the
haemagglutinin susceptible to a wider range of proteases. Since that outbreak,
no more cases have occurred.
2003 Onwards
The virus resurfaced in Feb 2003 to cause 2 infections (one fatal) in a Hong Kong family who had recently traveled to China. It began to cause outbreaks in the rest of Asia that year that were unnoticed. In 2004, Vietnam and Thailand started reporting human infections, followed by Cambodia, Indonesia and China in 2005. The strains exhibited divergence in these localities. It is now thought that highly pathogenic H5N1 is now firmly endemic Asia and has also spread to Europe and Africa. The WHO has put great priority and resources in the surveillance of H5N1 infections worldwide in the hope of averting or diminishing the impact of a pandemic should a pandemic capable strain emerges. http://www.who.int/csr/disease/avian_influenza/en/
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
For the most up-to-date figures, please visit http://www.who.int/influenza/human_animal_interface/H5N1_cumulative_table_archives/en/
Risks of a pandemic
The present H5N1 strains do not have the ability to transmit efficiently between humans. To date, there had been no certain cases of human to human transmission although a few suspicious clustering of cases in families have occurred. It is thought an avian influenza may acquire this capability through either
Reassortment with human influenza viruses (1957 and 1968). Reassortments in 1957 (H1N1-H2N2), and 1968 (H2N2-H3N2) are thought to have occurred through an intermediary host such as the pig.
Gradual mutations, as suspected in the 1918 pandemic H1N1 strain. Direct infection of humans by H5N1 opens the possibility that reassortment can occur without an intermediary host.
Many experts believe that a pandemic was stopped in 1997 in Hong Kong by the culling of chickens. The bottom line is that nobody knows when and if a pandemic will arise out of the current H5N1 outbreaks.
Control Measures
A large number of control measures have been implemented or recommended against avian H5N1 infection, at both the animal and human level. These include increased surveillance of livestock, increased biosecurity to prevent contact between livestock and migratory birds, and also vaccination of livestock. At the human level, there is increased surveillance, stockpiling of tamiflu, and also the development of candidate vaccines.
In August 2005, WHO sent all countries a document outlining
recommended strategic actions for responding to the avian influenza pandemic
threat. Recommended actions aim to strengthen national preparedness, reduce
opportunities for a pandemic virus to emerge, improve the early warning system,
delay initial international spread, and accelerate vaccine development. Despite
an advance warning that has lasted almost two years, the world is ill-prepared
to defend itself during a pandemic. WHO has urged all countries to develop
preparedness plans, but only around 40 have done so. WHO has further urged
countries with adequate resources to stockpile antiviral drugs nationally for
use at the start of a pandemic. Around 30 countries are purchasing large
quantities of these drugs, but the manufacturer has no capacity to fill these
orders immediately. On present trends, most developing countries will have no
access to vaccines and antiviral drugs throughout the duration of a pandemic.
Other Avian Influenza Viruses
In 1999, there were reports of human infections by avian influenza A H9N2 in Hong Kong and in Mainland China. These cases have been associated with direct or indirect contact with infected live or dead poultry. However, all these cases were very mild and it is thought that the virus was unlikely to pose a large public health risk. Of more concern is avian influenza H7N9 virus because most infected patients have become severely ill with a high mortality rate (up to 25%). Human infection by H7N9 virus was first reported in China in 2013. Since then, there had been outbreaks every year in China. Most of the cases of human infection with this avian H7N9 virus have reported recent exposure to live poultry or potentially contaminated environments, especially markets where live birds have been sold. This virus does not appear to transmit easily from person to person, and sustained human-to-human transmission has not been reported. Laboratory testing shows that influenza antiviral medicines called neuraminidase inhibitors (e.g. oseltamivir, zanamivir) are effective against H7N9. Among people with H7N9 infection in China, some of those who received early treatment with neuraminidase inhibitors have developed milder illness than those treated later on.