Acyclovir
C. Some Commonly Used Antiviral Agents
1. Acyclovir
Acyclovir is a synthetic guanine nucleoside analogue. The initial step of phoshorylation to ACV monophosphate is preferentially carried out by viral thymidine kinase rather than cellular kinases. The monophosphate cannot leave infected cells so that more non-phosphorylated compound enters to make up for the depleted intracellular concentration, only to be converted to the monophosphate. In this manner, the drug accumulates in the herpes-infected cells rather than in the uninfected counterparts. The monophosphate is then phosphorylated to the di and tri-phosphate forms by cellular enzymes. ACV triphosphate is the pharmacologically active form of the drug. It inhibits herpes DNA polymerase with little effect on the host cell DNA polymerase. It also has some chain termination activity and thereby it behaves as a "suicide inhibitor"
|
Acyclovir |
|
Acyclovir resistant strains of HSV have mutations in either the viral thymidine kinase gene or the viral DNA polymerase. Acyclovir also has antiviral activity against other herpesviruses such as VZV, CMV and EBV, although the mechanism is not so well understood in these cases. Forscarnet is the preferred drug in the treatment of acyclovir-resistant strains.
2. Valacyclovir
Valacylovir is an ester of acyclovir that is well-absorbed. Its bioavailibility is 2-5* greater than acyclovir. It is used for the treatment and suppression of genital herpes infection.
3. Famciclovir
Famiciclovir is the prodrug of penciclovir which is the active form and a guanosine analog. It has a very high bioavailabiity of 77%. It is converted into penciclovir by a two step process. The first step occurs in the gut and the second step in the liver. It has a long half life in the gut. It has a higher affinity for HSV thymidine kinase than acyclovir but a lower affinity for HSV DNA polymerase than acyclovir. It acts as an inhibitor of viral DNA polymerase and also as a chain terminator. At present famciclovir is licensed for the treatment of shingles and the dosage is 250mg tds. It is also used for the treatment and suppression of genital herpes infection.
4. Ganciclovir
Ganciclovir is a guanine nucleoside chemically related to acyclovir. It acts as a chain terminator and subsequent termination of viral DNA replication. The active form is thought to be the triphosphate. CMV does not specify TK and the initial phosphorylation of ganciclovir is thought to be mediated by other cellular enzymes. Ganciclovir has potent in vitro activity against all herpesviruses, including CMV. It has some activity against other DNA viruses such as vaccinia and adenovirus. Ganciclovir is more active against CMV than acyclovir. Ganciclovir has been shown to be of value in treating severe CMV infections in the immunocompromized, especially in conjunction with hyperimmune immunoglobulin. Reversible neutropenia is the most frequent adverse reaction. Ganciclovir resistance has been reported in immunocompromised patients being treated for CMV disease and is thought to be due to lack of phosphorylation of the drug by CMV infected cells. A recent prospective study estimated that 8% of patients receiving ganciclovir for more than 3 months developed resistant CMV.
5. Ribavirin
Ribavirin is a synthetic triazole nucleoside and the active form is ribavirin triphosphate. It is not incorporated into the primary structure of DNA or RNA during cellular synthesis of nucleic acids. In the case of influenza viruses, it inhibits the 5' capping of viral mRNAs. It has also been shown to inhibit influenza viral RNA polymerase complex. It has further been postulated that ribavirin triphosphate inhibits several steps in viral replication and this phenomenon may explain the failure to detect viral isolates that are resistant to ribavirin. Ribavirin has been shown to possess activity against both DNA and RNA viruses in infected cells. It has been found to have activity against adenoviruses, herpesviruses, CMV. vaccinia. influenza A and B, parainfluenza 1, 2, 3, measles, mumps, RSV, rhinovirus. Ribavirin has made a major contribution to the therapy of children infected with RSV where is given as an aerosol in hospital. It has also been shown to be effective against influenza A and B. It has also been reported to be of value in the treatment of Lassa fever, hantavirus disease and hepatitis C.
6. Zidovudine (AZT)
AZT is a synthetic analogue of thymidine. It requires
conversion to the triphosphate form by cellular enzymes. It
inhibits viral reverse transcriptase by acting as a chain
terminator. Viral reverse transcriptase is 100 times more
susceptible to inhibition by zidovudine triphosphate than host
cellular DNA polymerase. Once incorporated into the viral DNA
chain, viral DNA synthesis is terminated as no more
phosphodiester bonds could be formed. AZT is active in vitro
against many human retroviruses, including HTLV-I and HIV. AZT is
currently indicated for the management of patients with HIV
infection who have impaired immunity. (T4 cell count of 400- 500
or less) AZT has been clearly shown to prolong the life of
individuals infected with HIV. It has also been shown to be of
benefit for the treatment of symptomless individuals although
this is controversial.
7. Lamivudine
Lamivudine is a potent reverse transcriptase inhibitor. It is generally well tolerated by patients. It now usually forms an essential component in the combination therapy of HIV patients. Recently, it had been approved for the treatment of chronic hepatitis B.
8. Forscarnet
Forscarnet is a pyrophosphate analog and unlike nucleoside analogues, forscarnet does not need to be activated by cellular or viral kinases. Forscarnet binds directly to the pyrophoshate- binding sites of RNA or DNA polymerases. Forscarnet is difficult to use as it must be given continuously intravenously via an infusion pump. It is used for the treatment of CMV retinitis in AIDS patients receiving AZT therapy, as it does not have overlapping toxicity with AZT. It is also used in the treatment of AZT resistant HSV infections. Its major adverse effect is on renal function.
9. Amantidine
this compound inhibit the growth of influenza viruses in cell culture and in experimental animals. Amantidine is only effective against influenza A, and some naturally occurring strains of influenza A are resistant to it. The mechanism of action of amantadine is not known. It is thought to act at the level of virus uncoating. The compound has been shown to have both therapeutic and prophylactic effects. Amantidine significantly reduced the duration of fever (51 hours as opposed to 74 hours) and illness. The compound also conferred 70% protection against influenza A when given prophylactically. Amantidine can occasionally induce mild neurological symptoms such as insomnia, loss of concentration and mental disorientation. However, these symptoms quickly developed in susceptible individuals and cease when treatment is stopped. The therapeutic and prophylactic activity of amantidine is now generally accepted and numerous analogues of this compound have been prepared. Rimantadine is not as effective as amantadine but is less toxic. One factor that limits the usefulness of amantidine and rimantidine is the rapid development of resistance of these molecules in 30% of patients. These resistant mutants have been reported to be as capable of being transmitted and causing disease as the wild virus.
10. Zanamivir
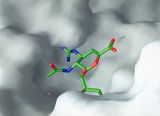
The rational approach to drug design has led to the design of
several potent inhibitors of influenza neuraminidase of which two,
zanamivir and oseltamivir are licensed for the treatment of
influenza A and B infections. In clinical trials, both agents
have demonstrated efficacy with minimal side effects. Because of
its poor bioavailibility, Zanamivir must be given by inhalation
whilst oseltamivir can be given orally. Because selection of drug-resistant
mutants characterized by changes in NA requires prolonged passage
in tissue culture, development of zanamivir-resistant viruses is
not expected to occur readily in patients. The available
information suggests that mutants may be less stable in vivo. The
significance of changes in hemagglutinin remains to be evaluated.
Overall the NA family of anti-influenza drugs is showing
considerable promise; resistant variants do not occur readily and
may be biological cripples.
|
3-D structure of neuraminidase |
Neuraminadse inhibitor zanamivir fitting into the neuraminidase molecule |
11. Immunoglobulins
Immunoglobulins are available in three different formulations; intramuscular form, IVIG, and hyperimmune globulins against individual viruses. Immunoglobulins are more effective when used prophylactically rather than therapeutically. Currently, HNIG is used primarily for the prevention of hepatitis A. HNIG can also be given to non- immunized contacts of measles. Hyperimmune globulins are used for the postexposure prevention of hepatitis B, chickenpox and rabies. It has also been used in the treatment of arenavirus infections, Crimean-Congo haemorrhagic fever and Rift valley fever. CMV Ig is given prophylactically to seronegative recipients of kidneys from seropositive donors. The use of prophylactic CMV Ig in BMT patients is controversial. CMV IVIG is used in conjunction with ganciclovir in the treatment of CMV pneumonitis. IVIG is also used in the treatment of chronic enteroviral meningoencephalitis in children with agammablobinaemia.
![]()
![]()
![]() Anti-HIV Compounds
Anti-HIV Compounds