Common colds account for one-third to one-half of all acute
respiratory infections in humans. they are responsible for a
considerable proportion of morbidity and economic loss each year
due to days lost from work. Rhinoviruses are responsible for 30%
of common colds, coronaviruses for 10%, adenoviruses,
enteroviruses, RSV, influenza, parainfluenza can also cause
common cold symptoms indistinguishable form those caused by
rhinoviruses and coronaviruses.
A. Properties
Belong to the family Picornaviridae
At least 100 serotypes are known
differ from enteroviruses in being acid-labile, having a high
buoyant density in caesium chloride, and grow optimally at 33
to 35oC.
Naked virus, ssRNA consisting of 7200 bp that make up 30% of
the mass of the virus particle.
Virus particle 28-32nm in diameter
Icosahedral capsid is made up of 60 copies of VP1, VP2, VP3,
and VP4. Canyons are found on each of the icosahedral faces
where cellular receptors bind.
Computer reconstruction of rhinovirus particle (Institute
for Molecular Virology)
B. Epidemiology
Rhinovirus infections occur worldwide. There are 2 seasonal
peaks of infection: one major peak during late summer and early
autumn, probably coinciding with the opening of schools, and a
second peak in Spring. A number of serotypes may circulate
simultaneously in a particular geographical area or community at
any one given time. Some serotypes may persist in a particular
community for several years. Other serotypes may disappear
completely form a community. It has been postulated that the
ecology of rhinoviruses include antigenic shift and drift.
Rhinovirus serotypes are numbered in chronological order of
discovery. In recent years, higher-numbered serotypes have
replaced lower-numbered serotypes as the predominant strains
circulating in the community in recent years. Some of the
untypable strains submitted as new prototypes appear to be
variants of lower-numbered strains.
Generally, it is estimated that an individual may suffer 2 to
5 episodes of colds per year. Infections are most common during
early life and generally decline with an increase in age,
probably due to the presence of antibodies against previously
encountered strains. Peak excretion of rhinoviruses occurs during
the acute phase of the illness. Close contact and crowding
appears to increase the transmission of rhinoviruses. Rhinovirus
appears to be transmitted mainly by the aerosol route, although
mechanical transmission by contaminated fingers or fomites into
the nasal epithelium or conjunctiva may also play a part.
The primary site of rhinovirus infection is in the nasal
epithelium. Virus may be detected in the nasal washings of
volunteers 24 hours after inoculation and reach a maximum peak by
the second or third day. The titres then start to decline and the
virus is usually undetectable by the fifth day. Symptoms of cold
appears one day after inoculation and peak on the third or fourth
day. It is uncertain whether rhinitis is due to the direct
cytocidal effect of virus replication or through the release of
mediators. Histamine have not been shown to play any role in the
development of rhinitis. Kinins, however, are found in elevated
quantities. Volunteers given kinins intranasally develop cold
symptoms.
Following infection, a specific humoral response is found in
both serum and nasal secretions. Serum-neutralizing antibodies do
not appear until 14 days after infection and thus recovery is
probably not mediated by antibodies. Serum antibodies remain
elevated for many years and are probably responsible form
protecting the person against reinfection. However, local
neutralizing antibodies are lost after 2 years.
D. Clinical Symptoms
The common cold is characterized by rhinorrhoea, nasal
obstruction, sneezing, sore throat and cough. There is little
fever and systemic reactions are uncommon. The illness may last
for a week or more. Otitis media and sinusitis may complicate
rhinovirus infection in a small proportion of patients (<1%),
usually in conjunction with a bacterial infection. The exact role
of rhinoviruses in the development of otitis media is not clear.
Rhinovirus infections also induce the onset of asthmatic attacks
in atopic individuals. Very rarely, rhinovirus infections are
associated with cough, chest pain, bronchiolitis and
bronchopneumonia. The general opinion is that rhinoviruses are
not a significant cause of croup, bronchiolitis , or viral
pneumonia.
Usually, a common does not require laboratory investigation.
If required, the diagnosis is generally made by the isolation of
the virus in a sensitive cell culture. Nasal washings are the
best specimens and should be collected early in the disease when
maximal titres of virus is excreted.
Virus isolation - Rhinoviruses are best isolated
in human embryo lung fibroblasts eg. MRC-5, or a
sensitive continuous cell line such as Ohio HeLa. Samples
should be inoculated into triplicates and rolled at 33oC.
The virus CPE, which consists of the rounding of cells
similar to that induced by enteroviruses should appear
within 8 days of inoculation. The identity can be
confirmed by acid lability tests. (pH3)
Direct detection of rhinovirus antigen - an ELISA
has been developed for the detection of rhinovirus
antigen in nasal washings.
Serology - virus neutralization tests remain the
best method. ELISAs have been described.
F. Treatment_and_Prevention
Early attempts to prevent rhinovirus infections by vaccination
have not been successful. The diversity of rhinovirus serotypes
and the lack of cross-protection during reinfection with
heterologus serotypes makes prevention by vaccination unlikely to
succeed. Attention has therefore focused on the development of
antiviral molecules such as interferons and synthetic anti-
rhinovirus compounds which could be used therapeutically as well
as prophylactically.
Prophylaxis - Natural and recombinant interferon have
been shown to be effective in preventing both infection and
illness when given intranasally in volunteers over short periods
of time. However, prolonged administration resulted in
considerable local cytotoxicity reactions eg. nasal irritation,
ulceration and bleeding. It is clear that interferons can not be
used for long periods, although they may considered for use over
short periods eg. 1 week to prevent an infection within the
family setting. Given this way, no side effects were reported in
volunteers. A number of synthetic compounds have been developed
which have potent anti-rhinovirus effects in vitro. One of these
compounds, R61837 was shown to be effective in vivo when it
significantly suppressed the appearance of colds in volunteers
given this compound prophylactically.
Treatment - Clinical trials with interferons failed to
modify the course of rhinovirus colds. A recent trial with R61837
again failed to modify the course of a clinical rhinovirus cold.
Because of the multiplicity of serotypes, it would be very
difficult to develop an effective vaccine against rhinoviruses.
Therefore the pursuit of antiviral agents remains the best
option.
Human coronaviruses were first isolated in the mid 1965 from
volunteers at the Common Cold Unit. The coronaviridae are a
monogeneric group of RNA-containing viruses that are associated
with respiratory infections in animals, including pigs, cats,
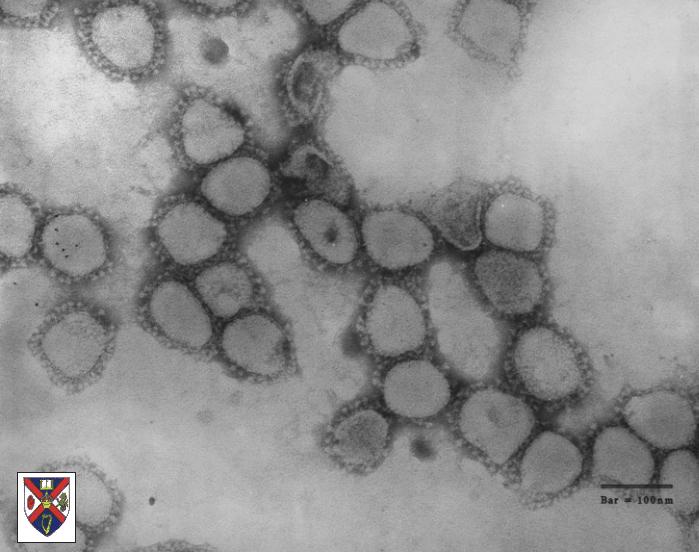
dogs, mice and chickens. The group was so named because of the
crown-like projections on its surface. At present, at least 10
species are recognized, of which human coronavirus is one. The
other are found in animals.
A. Properties
ssRNA enveloped viruses of pleomorphic morphology
60 to 220nm in diameter.
Positive stranded RNA; helical symmetry
characteristic club-shaped projections of 20nm, involved in
neutralization, fusion and in some coronaviruses,
haemagglutination.
Electronmicrograph of corona virus particles.
Some Human Coronavirus strains, namely 229E and serologically
related strains, are generally readily propagated in human cell
culture. However, other human coronavirus strains, namely OC43
and some serologically related strains, are considerably more
difficult to propagate in cell culture. Three antigenic molecules
are found in the virions ie. nucleocapsid, surface projection and
transmembrane proteins. The NP antigens may be common to all
coronaviruses, while the main antigenic determinants of
individual viruses reside on the surface projections. The surface
projection antigens are used for the serological grouping of
coronaviruses. One avian and two mammalian serological groups
have been established. Human coronavirus strains fall into each
of the mammalian groups which are named the OC43 and 229E
serological groups. It is not clear how closely related are the
viruses within a serological group.
B. Epidemiology
Generally, human coronavirus infections occur during the
winter and early spring but the peak period may vary by several
months. The periodicity of infections caused by 229E and OC43
group viruses follows a complex pattern, although they usually
cycle with an interval of 2 or 3 years. In general, high
infection rates in any particular year are caused by either 229E
or OC43 group viruses with only the occasional sporadic human
coronavirus infection belonging to the other group. This pattern
is observed throughout the world.
C. Clinical Features
Human coronaviruses are responsible for 10 - 30% of all common
colds. All age groups are affected, and infection rates have been
shown to be uniform for all age groups. This is different from
other respiratory viruses such as RSV, where there is a distinct
decrease in infection rates with an increase in age. The
incubation period is short, being 2 to 4 days. Infection may also
be subclinical or very mild. There have been some reports of more
severe lower respiratory tract involvement in young children and
old people. Reinfection of individuals with the same human
coronavirus serotype often occurs within 4 months of the first
infection, suggesting that homologous antibodies are protective
for only 4 months. Although many people have high antibody levels
after infection, reinfection with the same or related strains is
common. Antibodies to one human coronavirus group may not be
protective against infection with viruses from another group.
There are no differences in pathology observed between the OC43
and the 229E strains.
Other possible infections - coronavirus-like particles
are often seen in the faeces of children and adults suffering
from diarrhoea. These particles have a different morphological
appearance to those seen in respiratory infections. As yet, there
is no firm evidence associating the presence of these particles
to diarrhoea. Also human coronavirus particles have been observed
in tissue form patients suffering form multiple sclerosis, there
is no evidence for an aetiological role.
Diagnosis of human coronavirus infections is not attempted in
many routine laboratories. They have fastidious growth
requirement in cell culture, and the conditions caused by them
are of minor clinical significance. The routine diagnostic
procedures comprises of cell culture and serology.
Virus isolation - 229E and related strains can be
isolated in roller culture monolayers of human embryonic lung
fibroblasts, such as W138 and MRC5 cells. A virus CPE of small,
round, granular cells is seen throughout the monolayer. Isolates
can be confirmed by virus neutralization tests. OC43 related
strains usually cannot be grown in cell cultures. Isolation has
to be performed on organ cultures of human embryonic tissue such
as trachea.
Serology - virus neutralization are the most frequently
used tests. HI, CF and ELISA tests have been used. Most of these
tests are not carried out in routine diagnostic laboratories.
There is little, if any, antibody cross-reaction between strains
of 229E and OC43.
Direct detection of virus - indirect immunofluorescence
and ELISAs have been developed to detect the presence of
coronavirus antigen in nasal secretions with differing results.
The usefulness of indirect immunofluorescence has still to be
established.
No antiviral drugs against coronaviruses are available and
little research is being taken to produce any. However, vaccines
against certain animal coronaviruses are available.
The SARS crisis of 2003 was an instance when vigorous
international cooperation and intervention may have successfully prevented a
global health crisis. It fully showed the value of the WHO influenza
surveillance network. During the near pandemic between November 2002 and July
2003, with 8,096 known infected cases and 774 deaths (a mortality rate of 9.6%).
Here are the key events of the crisis. Local outbreaks of SARS infections were
reported in China, Hong Kong, Taiwan, Vietnam, Singapore, Philippines, Mongolia,
Canada, and the USA. A number of dead-end sporadic cases were reported in other
countries who received infected visitors from affected countries.
Identification of SARS. In early Feb 2003,
Guandong province in China reported 305 cases and 5 deaths caused by
atypical pneumonia of unknown cause. It later transpired that Guandong
was already having similar cases as early as Nov 2006. On the 19th Feb
2003, the WHO influenza network activated emergency pandemic plans after
receiving a report from Hong Kong confirming a case of Influenza H5N1
infection. This proved to one of the defining events in the control of
the SARS outrbreak. On the 21st Feb, a Chinese medical professor came to
Hong Kong to attend a relatives wedding. He stayed at a room on the 9th
floor of the Metropole Hotel. Six people who stayed on the same floor of
that hotel were infected and they carried the infection to the rest of
Hong Kong, Vietnam and Canada. Therefore all the cases outside China
could be traced to that event. In early March - Carlo Urbani identified
SARS (Severe Acute Respiratory Syndrome) as a unique clinical entity in
patients who had been infected by patient in a Vietnam hospital. That
patient had previously stayed on the 9th floor of the Metropole hotel.
WHO was put on alert. Sadly, Urbani himself later became infected and
died.
Discovery of SARS Virus. Initially, a number
of agents were implicated as the causative agent, including chlamydia,
metapneumoviruses, and influenza H5N1 but it soon became apparent that a
new agent may be involved. The breakthrough came on 21st March when the
Hong Kong university reported the isolation of an unknown virus in FRhk4
cells, and were able to demonstrate a rising antibody response against
this virus by IF in patients with SARS. Furthermore, virus-like
particles were seen in lung biopsies. On 22nd March, CDC reported the
growth of a corona-like virus in Vero E6 cells. This was identified as a
new coronavirus and PCR based diagnostic tests became rapidly available.
Properties or SARS Virus
The SARS virus is a novel coronavirus that did not
belong to the previously known OC43 and 229E serogroups. It had a genome
of 29,000 bases. It had some rather unusual virological aspects.
Incubation period:- mean 6.37
(95% CI 5.29-7.75)
Risk of transmission is
greatest around day 10 of illness when maximum excretion of the
virus occurs in respiratory secretions and faeces.
No evidence that patients can
transmit infection 10 days after fever has resolved.
The virus appeared to be
endemic in bats, where they do not cause any disease. The jump to
human appeared to have occurred via Civet cats, which is a delicacy
in Southern China.
Epidemiology
Incubation around 6 days.
Spread by droplets – there is no evidence it is an
airborne disease. It is not certain whether faecal-oral spread can
occur.
Health care workers were at special risk, especially
those involved in procedures that may generate aerosols. In some cases,
transmission to health care workers occurred despite that the staff was
wearing full protection. The fact that medical staff is at special risk
is probably due to the fact that maximum excretion of the virus occurs
more than one week after the onset of symptoms, when the patient is
likely to be in hospital.
Risk of transmission is greatest at around day 10 of
illness when maxi
No evidence that patients can transmit infection 10
days after fever has resolved.
Children are rarely affected
by SARS
The implications of the
Metropole Hotel are not yet fully understood.
Risk of in-flight transmission
– 5 international flights had been associated with the transmission
of SARS. No evidence of in-flight transmission after the 27 March
2003 WHO advisory on flights.
Super-spreading Events. The SARS virus is not
normally highly infectious but certain individuals have spread the virus to
a large number of individuals. These individuals were already known as
super-spreaders but the WHO now prefer to call them super-spreading events.
In Hong Kong, 3 super-spreading events are known to have occurred.
Metropole Hotel - this is not fully understood.
Prince of Wales Hospital - the patient was an asthmatic who was put on a
nebulizer. It is that that the nebulizer allowed the virus to travel much
wider and further than it would normally do.
Amoy Garden - this is perhaps the most spectacular event of the whole
crisis. 321 persons in the housing estate were infected. Residents of
affected blocks were first quarantined in their homes and then
transferred to internment camps. The clustering of cases suggested that
a defective sewage system was probably responsible.
Diagnosis
The initial diagnosis of SARS was clinical. According to the
guidelines issued by the WHO, SARS may be suspected
in a patient who has:
Any of the symptoms including a fever of 38 °C
(100.4 °F) or more AND
Either a history of Contact (sexual or casual) with
someone with a diagnosis of SARS within the last 10 days
OR Travel to any of the regions identified by the
WHO as areas with recent local transmission of SARS
(affected regions as of 10 May 2003 that were parts of
China, Hong Kong, Singapore and the province of Ontario,
Canada).
A probable case of SARS has the above findings
plus positive chest x-ray findings of atypical pneumonia or
respiratory distress syndrome.
With the advent of diagnostic tests for the
coronavirus probably responsible for SARS,
the WHO has added the category of
"laboratory confirmed SARS" for patients who
would otherwise fit the above "probable"
category who do not (yet) have the chest
x-ray changes but do have positive
laboratory diagnosis of SARS based on one of
the approved tests (ELISA,
immunofluorescence or PCR).
A battery of laboratory tests became rapidly available on
the discovery of the SARS virus.
RT-PCR - This is the mainstay of diagnosis of SARS
infection. A variety of specimens can be used including NPA (preferred),
throat swabs, trachael aspirates, and faeces.
Virus Isolation - Vero E6 and FRhk4 cells may be
used. However, the positivity rate is much lower than PCR and stringent
Biosafety Level III facilities are required. Therefore, this is not
recommended for small routine laboratories.
Serology - SARS virus infection may be confirmed
by seroconversion or rising titres of antibodies. IFT and ELISAs are
available but originally, whole virus antigen was used which required
biosafety level III facilities. Because of the low predictive value of the
first generation PCR assays, a serological diagnosis was often the only
means of confirming a diagnosis of SARS.
Treatment
A number of treatments were tried initially including
ribavirin and steroids. However there is little evidence to suggest that any
therapies used during this period was effective. In 2004, it was reported
that researchers in China had successfully produced a vaccine that induced
antibodies in 24 out of 36 volunteers but more research will be needed to
ascertain whether it would be effective.
Post Epidemic
Since
July 2003, laboratory acquired cases of SARS had been reported in
Singapore, Taiwan and China. These have occurred in Biosafety level III
and IV laboratories. Sloppy practices and procedures were to blame
rather than failings in the containment equipment. In Jan 2004, a 32 old
male with diagnosed with naturally acquired SARS in Guandong, China. He
infection was linked to contact with civet cats and the Chinese
authorities promptly ordered the slaughter of 10,000 civet cats and
related species of animals in the area.
MERS Virus
Middle East respiratory syndrome (MERS) is a
viral respiratory disease caused by a novel coronavirus (Middle East
respiratory syndrome coronavirus, or MERS‐CoV) that was first identified
in Saudi Arabia in 2012. It has since spread to several countries. Most
people identified as infected with MERS-CoV developed severe acute
respiratory illness, including fever, cough, and shortness of breath.
Pneumonia is common but not always present. Diarrhoea has also been
reported in some patients. Approximately 35% of reported pateients with
MERS have died. There are asymptomatic cases of MERS infection but they
are in the minority. The majority of human infections occur through
human to human transmission in health care settings. It is thought that
camels act as reservoirs for the MERS virus. The virus does not pass
easily between humans but several outbreaks have occurred in health care
settings in Saudia Arabia, UAE and S. Korea. Since 2012, 27 countries
have reported cases of MERS virus infection. Laboratory diagnosis mainly
depends on the detection of MERS virus DNA from blood and respiratory
secretions. There is no specific treatments available at present.